Rheumatoid Arthritis in the Cervical Spine
Danny F. Searcy
Charles W. Cha
Scott D. Boden
Charles R. Clark
Rheumatoid arthritis in the cervical spine results in anatomic abnormalities as a consequence of the destruction of synovial joints, ligaments, and bone. Inflammatory synovitis can produce erosion of both bone and ligament, resulting in pain, instability, bony subluxations, and ultimately spinal cord or brainstem compression. Compression of the cervical spinal cord and/or brainstem may result from either direct compression by synovial pannus or indirect compression due to cervical subluxations. Atlantoaxial subluxation is attributed to erosive synovitis in the atlantoaxial, atlantoodontoid, and atlantooccipital joints, as well as the synovium-lined bursa between the odontoid and the transverse ligament. Atlantoaxial impaction (cranial settling, upward translocation of the odontoid, pseudobasilar invagination, vertical subluxation) describes the settling of the skull on the atlas, and the atlas on the axis, resulting from erosion and bone loss in the occipitoatlantal and atlantoaxial joints. Subaxial subluxations occur through destruction of the facets, interspinous ligaments, and intervertebral disks (spondylodiskitis).
Although much is known about the natural history, pathophysiology, pharmacologic management, and operative stabilization of patients with rheumatoid disease in the cervical spine, the clinically relevant question of when to undertake operative intervention in the cervical spine remains somewhat unclear. Operative stabilization or arthrodesis has traditionally been reserved for patients with severe progressive neurologic deficit or intractable pain (1). The early experience with many of these patients demonstrated a high operative morbidity as well as variable neurologic recovery once notable paralysis had occurred.
To complicate the operative decision further, although many patients have radiographic evidence of cervical spine involvement, not all have progression of their cervical disease and develop paralysis. Therefore, a difficult clinical question remains: How can we identify patients before they develop irreversible neurologic deficit and when should we proceed with operative stabilization in this select group? Although the answer to this question still remains unclear, some light may be shed on the subject by examining what is known about predictors of paralysis as well as predictors of the potential for neurologic recovery after operations in patients with rheumatoid disease in the cervical spine. After such an analysis is undertaken, a rational scheme can then be devised to monitor patients safely and costeffectively, to decide when secondary neurodiagnostic imaging studies should be performed, and, last, to offer recommendations for the timing of operative stabilization. Because the techniques of operative stabilization are covered in the chapters that follow, this chapter focuses primarily on developing a strategy for timely and cost-effective evaluation and management of these challenging patients.
PREDICTORS OF PARALYSIS
NATURAL HISTORY
Defining the natural history of a particular disease is important because it serves as a baseline from which one
can gauge the potential of certain therapeutic modalities to alter or impact the natural course of a disease process. Unfortunately, with chronic diseases such as rheumatoid arthritis, establishing the natural history of the disease can be problematic for several reasons. First, gauging the natural progression of a disease requires long-term prospective studies that follow untreated patients. In situations where effective therapies are known, it is unethical to hold those beneficial therapies for the sake of research. Secondly, the logistics of completing these long-term studies can be complicated. As a result, knowledge of the natural history of cervical spine pathology in the rheumatoid patient is limited. Only a few studies address this topic, and current knowledge is based on smaller, retrospective evaluations.
can gauge the potential of certain therapeutic modalities to alter or impact the natural course of a disease process. Unfortunately, with chronic diseases such as rheumatoid arthritis, establishing the natural history of the disease can be problematic for several reasons. First, gauging the natural progression of a disease requires long-term prospective studies that follow untreated patients. In situations where effective therapies are known, it is unethical to hold those beneficial therapies for the sake of research. Secondly, the logistics of completing these long-term studies can be complicated. As a result, knowledge of the natural history of cervical spine pathology in the rheumatoid patient is limited. Only a few studies address this topic, and current knowledge is based on smaller, retrospective evaluations.
Reports documenting the prevalence of cervical subluxations in the rheumatoid population vary widely. From 43% to 86% of rheumatoid patients have radiographic evidence of cervical instability (2). The most common type of cervical subluxation in rheumatoid patients is atlantoaxial subluxation, which represents 65% of all cervical subluxations (Fig. 60.1). Of patients with atlantoaxial subluxation, most have anterior subluxation, although approximately 20% may have lateral subluxations and less than 10% have posterior subluxation. Rotatory subluxations have been reported but are rare (3). Approximately 20% of rheumatoid subluxations involve basilar invagination (cranial settling) alone or in combination with atlantoaxial subluxation. About 15% of rheumatoid patients with cervical subluxations may also have subaxial subluxation, which frequently occurs at multiple levels. Rheumatoid patients may present with any combination of these three main types of cervical instability.
 Figure 60.1. Lateral radiograph of the upper cervical spine showing atlantoaxial instability (A), CT myelogram shows spinal cord deformation (B), and MRI reveals the myelomalacia that has developed from the chronic compression (C). |
Despite the high prevalence of radiographic changes observed in the rheumatoid cervical spine, associated neurologic deficits are reported to occur in only 7% to 58% of patients (4,5). The wide variation in the reported prevalence of neurologic deficits can be attributed to the variability in the neurologic classification systems as well as to the difficulty in detecting subtle neurologic changes in this group of patients. Regardless, it is clear that many patients with pain and radiographic changes do not display a neurologic deficit.
In order to better characterize the natural history of cervical disease in the rheumatoid population, studies have evaluated the rate of progression for both radiographic as well as neurologic changes. Rana (6) followed the radiographs of 41 patients with atlantoaxial instability for a period of 10 years. Twenty-seven percent of these patients were noted to have radiographic subluxations that progressed. While 61% showed no radiographic changes and 12% actually improved radiographically. In 1981, Pellicci et al. (7) noted that although 80% of their patients with rheumatoid arthritis who had cervical involvement demonstrated radiographic progression, only 36% had
neurologic progression. Boden et al. (8) evaluated the clinical course of 73 patients for an average of 7.1 years. Of the 73 patients, 42 (58%) developed paralysis. The majority of these patients were treated operatively; however, seven were treated nonoperatively because they either refused surgery or had medical contraindications to surgery. Six of seven patients had a deterioration of neurologic function, and all were dead within 4 years of onset of paralysis. Five of the seven deaths could be directly attributed to the cord compression.
neurologic progression. Boden et al. (8) evaluated the clinical course of 73 patients for an average of 7.1 years. Of the 73 patients, 42 (58%) developed paralysis. The majority of these patients were treated operatively; however, seven were treated nonoperatively because they either refused surgery or had medical contraindications to surgery. Six of seven patients had a deterioration of neurologic function, and all were dead within 4 years of onset of paralysis. Five of the seven deaths could be directly attributed to the cord compression.
These studies indicate that though rheumatoid patients are likely to have radiologic progression of their cervical disease, the majority will not go on to develop a neurologic deficit. However, once paralysis develops, the natural history seems to be one of progressive neurologic deterioration, which ultimately can lead to death. In fact, sudden death in the rheumatoid patient with cervical involvement is a substantial concern and occurs secondary to medullary compression caused by upper cervical instability. Postmortem analyses indicate that sudden death from medullary compression can occur in as high as 10% of patients (2).
Our knowledge of the natural history of rheumatoid cervical disease indicates that a wide variation exists in radiographic measurements. There is also a significant amount of overlap between symptomatic and asymptomatic patients. These factors combine to make the radiographic definition of instability elusive in this patient population. Furthermore, the poor correlation of neurologic symptoms with radiographic evidence of instability makes the identification of an impending neurologic deficit, and therefore the ideal candidate for surgical treatment, difficult.
In order to better identify the rheumatoid patient with an impending neurologic deficit, investigators have evaluated certain clinical and radiographic parameters for predicting patients at a higher risk for neurologic compromise.
CLINICAL PRESENTATION
The findings that accompany cervical involvement with rheumatoid arthritis can be very subtle. A careful history and physical examination are crucial in the spinal evaluation of the rheumatoid patient. Typically, these patients manifest with pain, frequently at the craniocervical junction. Patients may also complain of occipital headaches, which may be secondary to an occipital neuralgia precipitated by compression of the greater occipital branch of C2. If the greater auricular branch is involved, then the patients may develop ear pain. Compression of the trigeminal nucleus with vertical settling can present as facial pain. Neurologic symptoms are multiple and can be vague ranging from paresthesias in the hand to Lhermitte phenomena, which is an electrical sensation traveling through the body. Vertebrobasilar insufficiency, which is associated with basilar invagination, may cause tinnitus, vertigo, loss of equilibrium, and visual disturbances. Diplopia, dysphagia, and urinary dysfunction, frequency or retention, are important warning signs that are caused by bulbar involvement. Vertical nystagmus and Cheyne-Stokes respirations can be associated with brainstem compression. Joint crepitation and instability may be palpated in the upper cervical spine and noted with range of motion sometimes in the form of a “klunk.”
Physical examinations may be difficult to interpret in this population because subtle neurologic changes may be masked for a variety of reasons and are often confused or misattributed to other musculoskeletal manifestations of this disease. For example, motor strength testing may be difficult in the patient with multiple joint deformities and tendon subluxations or ruptures. These patients typically have a baseline weakness due to muscular atrophy. Peripheral nerve entrapment may also confuse the neurologic examination. Detection of long tract signs, which herald the onset of early myopathy, can be very difficult given all of the peripheral involvement that can occur with this disease. Therefore, the clinician must be astute in detecting the subtle changes that accompany neurologic compression of the cervical spine.
Studies have evaluated the use of certain clinical parameters to help predict which patients are at risk of developing progressive cervical disease and neurologic deficit. The clinical risk factors that have been identified include: male gender, severe peripheral disease, the use of corticosteroids, and age of onset of disease (2,9,10). It is difficult to determine whether or not the use of corticosteroids is truly an independent risk factor rather than just an association with patients with severe peripheral disease. A study of 149 patients attempted to correlate laboratory values with the development of cervical spine subluxations in the rheumatoid population. Subluxation in the cervical spine was associated with the presence of HLA-DW2 and HLA-B7 cross-reacting group. Using these laboratory values along with the age of onset of disease, the researchers were able to successfully predict radiologic outcome in 82% of the patients (11). Unfortunately, these clinical parameters that include history, physical examination, and laboratory evaluation are only a moderate help at predicting which of these patients are at risk for developing a neurologic deficit.
RADIOGRAPHIC PREDICTORS OF PARALYSIS
Clinicians must often rely heavily on expensive, often invasive, and less than perfect imaging studies to identify the patient that is at risk of developing a neurologic deficit. Prediction of the timing of onset of myelopathy in any given patient is difficult, not unlike predicting an earthquake before it occurs. Studies of large populations of rheumatoid patients have enabled the establishment of parameters for predicting patients at higher risk for neurologic compromise.
PLAIN RADIOGRAPHY
Plain radiographs are the basis of radiographic evaluation of the rheumatoid cervical spine. Although magnetic resonance imaging (MRI) is the superior imaging modality for demonstrating cord compression from subluxation or synovial pannus, it is expensive, somewhat time-consuming, and therefore not practical to use on a routine or ongoing
basis to screen all patients with rheumatoid arthritis. Therefore, it is important to review plain radiographs and to assess what can and cannot be learned from such studies. Ventral atlantoaxial subluxation may be assessed on a lateral cervical spine radiograph by measuring the anterior atlantodental interval (AADI) from the middorsal margin of the anterior ring of C1 to the ventral surface of the odontoid. If this interval measures more than 3 mm in an adult or 4 mm in a child, it is considered abnormal and spinal cord function may be in jeopardy. The interval is generally accentuated on a flexion view if instability or excessive motion is present. In fact, the amount of dynamic motion present at the atlantodental interval, measured as the change between flexion and extension, may be more clinically relevant than the maximal interval on a single flexion view.
basis to screen all patients with rheumatoid arthritis. Therefore, it is important to review plain radiographs and to assess what can and cannot be learned from such studies. Ventral atlantoaxial subluxation may be assessed on a lateral cervical spine radiograph by measuring the anterior atlantodental interval (AADI) from the middorsal margin of the anterior ring of C1 to the ventral surface of the odontoid. If this interval measures more than 3 mm in an adult or 4 mm in a child, it is considered abnormal and spinal cord function may be in jeopardy. The interval is generally accentuated on a flexion view if instability or excessive motion is present. In fact, the amount of dynamic motion present at the atlantodental interval, measured as the change between flexion and extension, may be more clinically relevant than the maximal interval on a single flexion view.
Ventral atlantoaxial subluxation may also be assessed by measurement of the posterior atlantodental interval (PADI), which is measured from the dorsal aspect of the odontoid to the ventral margin of the C1 lamina. This interval does not represent the space available for the spinal cord in patients with rheumatoid arthritis because the retro-odontoid synovial pannus may occupy 1 to 3 mm or more of that space.
Vertical migration of the odontoid can be assessed radiographically in a variety of ways (Fig. 60.2). McRae’s line connects the front of the foramen magnum to the back, and the odontoid should not project above this line. The upper tip of the odontoid process normally lies 1 cm below the ventral margin of the foramen magnum. Chamberlin’s line is drawn from the dorsal margin of the hard palate to the dorsal margin of the foramen magnum. The tip of the odontoid should not project more than 3 mm above this line; projection 6 mm above this line is considered pathologic. Commonly, however, the margins of the foramen magnum are difficult to define without a tomogram. McGregor’s line is easier to use because it connects the posterior margin of the hard palate to the most caudal point of the occiput. The tip of the odontoid should not project more than 4.5 mm above this line.
Because the odontoid tip may be difficult to identify, particularly with rheumatoid-related osteopenia or destruction, another measurement was described by Redlund-Johnell and Petterson (12). McGregor’s line is drawn on a lateral cervical radiograph with the head in neutral position. The distance to the lower end plate of the C2 vertebral body is then measured. Less than 34 mm in men and less than 29 mm in women is defined as vertical migration of the odontoid. Clark et al. (13) have described the so-called station of the atlas that notes the relationship between the anterior arch of the atlas and the axis. Normally, the atlas lies adjacent to the upper portion of the dens. If the arch lies adjacent to the base of the dens or body of the axis, moderate to severe cranial settling may be present. Ranawat criterion measures the distance between the center of the second cervical pedicle and the transverse axis of the atlas along the axis of the odontoid process. A measurement of less than 15 mm in males and less than 13 mm in females is indicative of basilar invagination (14). All these measurements, as well as others (15,16), attempt to identify and quantitate the degree of odontoid encroachment on space normally occupied by the brainstem and spinal cord.
 Figure 60.2. Schematic (lateral view) of upper cervical spine showing some of the reference lines for measuring basilar invagination. |
Vertical migration of the odontoid is uncommon but is believed to be the most dangerous cervical abnormality in the rheumatoid patient. Plain film radiography can be a valuable tool in evaluating rheumatoid changes but poses a challenge with sensitivity and negative predicative values. No measurement evaluating plain film radiography has a sensitivity rating higher than 90%, which is the desired sensitivity for any plain radiographic criterion used to screen for basilar invagination. However, by using a combination of measurements described by the Clark station, Redlund-Johnell criterion and the Ranawat criterion give the best predictability. If all three of these tests are negative, there was a 91% chance that the patient did not have invagination. This combination also provided a high sensitivity (94%) suggesting that very few patients with this disease would be missed (17).
Subaxial subluxations tend to occur at multiple levels in a given patient, producing a “staircase” or “stepladder” deformity (Fig. 60.3). Lack of osteophyte formation is typical of rheumatoid arthritis, as is involvement of C2 to C3 and C3 to C4, which are not commonly involved in degenerative disease. Subaxial subluxation may be quantitated on lateral cervical radiographs as relative translation with the distance of the forward slip (in millimeters) expressed as a percentage of the total anteroposterior diameter of the inferior vertebral body. Alternatively, this deformity may be described by measuring the minimum spinal canal diameter behind the slipped vertebra. The latter measurement may more closely reflect potential spinal cord compression. Ascertaining whether the subluxations are fixed or mobile on flexion-extension radiographs is also important.
In evaluating cervical spine radiographs in the rheumatoid patient, close attention should be focused on the superior facet joints. Resorption of the superior facet is considered the most important predicative factor in development of subaxial subluxation and subsequent myelopathy. Matsumoto et al. (18) describe various stages of superior facet absorption in the subaxial cervical spine and determine this as an important factor in the development of myelopathy. Four stages of facet resorption are described with stage 0 being a normal facet joint. Stage 1 (erosive), the facet joint has a slight or medium macroscopic erosive change. Stage 2 (tapering type), the facet joint has
severe destructive changes as the superior facet looks like a tapering pencil. Stage 3 (resorptive type), there is severe involvement of the facet joint. In addition, radiographic evidence of spinous process absorption in the subaxial cervical spine presents a heightened concern for the development of myelopathy (Fig. 60.4).
severe destructive changes as the superior facet looks like a tapering pencil. Stage 3 (resorptive type), there is severe involvement of the facet joint. In addition, radiographic evidence of spinous process absorption in the subaxial cervical spine presents a heightened concern for the development of myelopathy (Fig. 60.4).
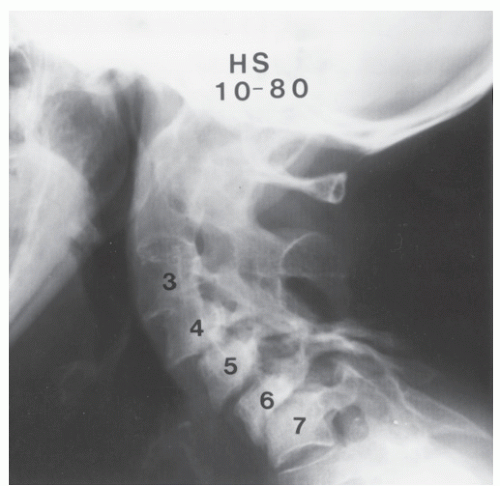 Figure 60.3. Lateral radiograph of a patient with rheumatoid arthritis with progressive multiple-level subaxial subluxations from the third through seventh cervical vertebrae. The patient developed slowly progressive cervical myelopathy and required surgery. (Reprinted with permission from Boden SD, Dodge LD, Bohlman HH, et al. Rheumatoid arthritis of the cervical spine. J Bone Joint Surg Am 1993;75:1282-1297.) |
An increasing number of studies assessing the measurements made from plain lateral cervical radiographs have shown that the AADI is unreliable at discriminating patients with rheumatoid arthritis from those without neurologic deficit. One example is a study by Collins et al. (19), which showed that 61% of rheumatoid patients undergoing total joint replacement operations had radiographic evidence of atlantoaxial instability, yet only 50% of patients had any signs or symptoms of their cervical disease. In some studies, investigators attempted to use the AADI as a potential criterion for recommending operative intervention in patients with rheumatoid arthritis affecting the cervical spine. Although the normal atlantodental interval is 3 mm, more than 5 mm of subluxation is considered to represent atlantoaxial instability (20). In studies of patients with rheumatoid arthritis, operative intervention for an atlantodental interval greater than 8 mm, greater than 9, or greater than 10 mm, depending on the series, has been recommended (6,10,13). Other investigators (21) have suggested that it is not the absolute amount of subluxation present but the degree of mobility that is most important. In addition, neurologic progression is generally considered inevitable once any degree of cord compromise is present. Unfortunately, there is poor correlation between vertebral subluxation on plain radiographs (measured by the AADI) and cord compression as shown by MRI (22).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


