Introduction
Focal motor seizures have been recognized since Hippocrates first noted them, beginning contralateral to the side of head injury. Hemiplegic epilepsy was first actually described by Bravais in 1827.62 Jackson pointed out that focal epileptic seizures were due to a “sudden and excessive discharge of gray matter in some part of the brain” and that the symptoms of the seizure depended on the “seat of the discharging lesion.” Fritsch and Hitzig demonstrated that electrical stimulation of the motor cortex in animals gave rise to focal muscular contractions in the contralateral limb.38 In 1887, Charcot proposed the term jacksonian epilepsy to describe seizures with a “march” of symptoms.59 Another term “Bravais-jacksonian seizures” has been used by some to indicate a similar march of symptoms. The term aura has been in use since Galen’s time; its literal meaning “breeze of air” refers to the altered sensations experienced by the patient with epilepsy at the start of a seizure. Erastus pointed out that an aura was the start of the seizure itself.48 Electrical stimulation of the brain100 and detailed observations of spontaneous and metrazol-induced seizures3 have provided much of the basis for our current knowledge of focal motor seizures.
Definitions
The International Classification of Epileptic Seizures divides simple partial motor seizures into those with or without a march, versive, postural, and phonatory seizures.30,31 Consciousness is retained during these seizures; however, occasionally, a seizure discharge may remain localized and still produce alterations of consciousness.46 The epileptogenic zone in the involved hemisphere may be very restricted or quite large, even though terms such as “partial” or “focal” are employed. A more recent seizure classification is based on clinical symptomatology and is independent of electroencephalographic (EEG), neuroimaging, and historical information. In this classification, terms such as focal clonic, focal tonic, or versive are used, and evolution during the course of the seizure is indicated by arrows, for example somatosensory aura → left arm clonic seizure → left versive seizure.8,81,82
Epidemiology
In a series of 8,938 patients admitted to the University Hospital of Lyon over a 10-year period from 1965 to 1975, 1,158 (12.9%) patients had focal motor seizures without march, 199 (2.2%) patients had focal motor seizures with march, 582 (6.5%) had hemiconvulsions, and 461 (5.2%) had adversive seizures.89 In a population-based study of 1,054 patients from Denmark, Wagner found that 17% of epileptic patients had simple partial seizures.124 Loiseau reported that out of 200 patients with partial seizures, 71 (35.5%) had partial motor symptoms, of whom 10 patients exhibited a march.76
Anatomic Pathways and Pathophysiology
Simple partial seizures with motor manifestations are due to ictal onset within or near the pre- and postcentral gyri of the contralateral hemisphere. The somatotopic motor and sensory representation of various regions of the body has been documented by the pioneering work of Penfield and Jasper100 and others75 (Fig. 1). It is believed that the relatively large representation of the face and fingers is accounted for by the majority of focal motor seizures starting in those brain regions. Holowach noted that 25 of 50 jacksonian seizures in children began in the face, 17 from the hand, 7 from the arm, and 9 from the leg.60 Penfield and Jasper also noted that the angle of the mouth was involved first in seizures affecting the face; upper-extremity seizures began in the thumb and index finger, whereas lower-extremity seizures often began in the great toe.100 Another factor is the seizure threshold of various regions of the homunculus—the trunk not only has the smallest cortical representation87 but also a higher threshold to electrical stimulation.37 Jacksonian seizures show an orderly “march,” beginning, for example, in the thumb, then involving other fingers, the wrist, forearm, proximal arm, shoulder, and then the face (usually the orbicularis region first). At times, the march may skip certain areas, perhaps because of different seizure thresholds in various regions.4 Sensory phenomena may occur in about one third of patients with focal motor seizures;27 this may be caused by involvement of pre- and postcentral regions by the epileptogenic lesion or preferential pathways for spread of the ictal discharge.36,112 Clonic seizures were reported in 29% of 24 patients with frontal lobe epilepsy.113 Noachtar and colleagues examined seizure phenomena preceding and following clonic movements in a group of patients with frontal lobe epilepsy: Clonic seizures were usually preceded by behavioral arrest or tonic movements and were the initial manifestation in one third.93 Motor symptoms also occur in seizures starting elsewhere and spreading to the sensorimotor cortex, such as the parietal lobe,114,126 occipital lobe,83,127 or even the temporal lobe.17
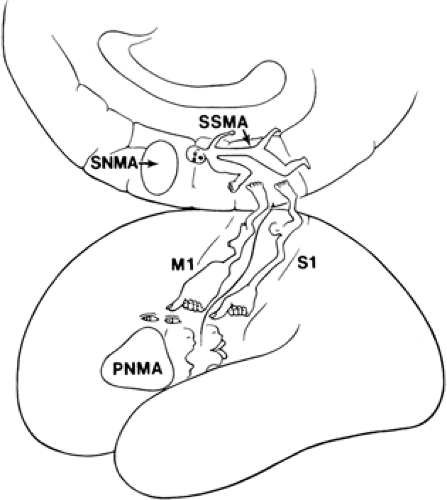 FIGURE 1. Motor and sensory homunculi. The lateral convexity homunculus was simplified from Penfield and Jasper (1954); the supplementary sensorimotor area (SSMA) homunculus was prepared based on stimulation findings by Lim et. al (1994). |
The output of the primary motor area (PMA) goes to the corticospinal and corticobulbar tracts, as well as to the supplementary motor area and homologous areas in the opposite hemisphere via the corpus callosum. The PMA gives rise to only one third of the corticospinal and corticobulbar tract fibers, another third come from the premotor cortex and supplementary motor area (SMA), while another third arise from the parietal lobe.5 Ictal single photon emission computed tomography (SPECT) scan findings in patients with frontal and parietal lobe epilepsy show good agreement with data from electrical brain stimulation studies and invasive EEG recordings.28,54,58,84,92
Very rarely, focal seizures have been reported in patients with cerebellar, brainstem, or spinal lesions.52,55 In Harvey’s patient, localized hyperperfusion on ictal SPECT and ictal discharges were noted in the vicinity of the lesion, and the seizures disappeared after surgical removal of the lesion.
Clinical Features
Ictal
The hallmark of simple motor seizures is focal motor activity that may be expressed as clonic, tonic, postural, or phonatory activity. The international classification of seizures divides simple partial motor seizures into clonic, tonic, postural, and phonatory seizures.30,31
Clonic seizures consist of jerky, usually rhythmic movements and are usually seen with seizures starting from the sensorimotor cortex. The clonic movements may remain restricted to one region or spread in a jacksonian manner. As mentioned earlier, jacksonian seizures begin and spread in characteristic ways. Hemiconvulsions are clonic seizures affecting one side of the body. These often occur in the setting of infantile hemiplegia.2,19,43,47 Most clonic seizures are brief, lasting less than 1 or 2 minutes. Focal myoclonus has also been reported in infants and young children with dysplastic lesions of the motor cortex.71
Persistent, stereotyped, periodic, or quasi-periodic clonic activity may occur, and different types are described.42 Kojevnikov gave the label epilepsia partialis continua (EPC) to repeated jacksonian seizures characterized by a march of clonic seizures. Between such attacks, patients have persistent, stereotyped focal myoclonic episodes.67 The twitching typically affects the thumb or big toe, and individual jerks occur no more than 10 seconds apart.119 Another type consists of repeated, stereotyped clonic seizures without a march. The usual etiology for EPC is a lesion involving the sensorimotor cortex resulting from stroke, tumor, trauma, metastasis, or hypoxic ischemic encephalopathy.98,119 EPC is frequently seen in the setting of Rasmussen encephalitis, in the subacute type of measles encephalitis, and in mitochondrial disorders such as mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS).22 EPC cases have also been reported in nonketotic hyperglycinemia affecting adults and in some patients with subcortical lesions.24
Tonic motor seizures produce sustained contraction of a limb and result in assumption of various postures. Tonic motor seizures are believed to implicate a wider area of cortex including the SMA and premotor region.34,44,100,128 The M2e posture described by Ajmone-Marsan is seen in seizures arising from the SMA region. It consists of abduction, elevation, and external rotation of the contralateral arm with the elbow slightly flexed; the head and eyes deviated as if to look at that arm, while both lower extremities may be slightly flexed at the hips and knees or extended. Even in patients where tonic posturing appears unilateral, a bilateral increase or decrease of tone occurs.1
Postural seizures refer to tonic contraction affecting more than one limb and the trunk or head—typically these are bilateral tonic movements affecting the proximal muscles more than the distal muscles. Rarely, motor seizures are manifested by focal weakness instead of tonic or clonic activity.45,51,100,122 Consciousness is retained during SMA seizures in 72% of attacks.3 A prolonged continuous or interrupted vocalization may occur in seizures involving the supplementary motor or lower rolandic area from either hemisphere.
Versive seizures are characterized by predominantly tonic contraction of head and eye muscles resulting in sustained, forceful deviation to one side (invariably contralateral).
Consciousness is often lost by the time a patient experiences version; at other times, however, patients are conscious of forced eye and head deviation;26,90 often the angle of the mouth is also deviated to the same side, and the neck is extended.63 In Wyllie’s study, version was accompanied by clonic or posturing arm movements or facial clonic movements on the side of contraversion. The versive movement was smooth in 65% and jerky in 35% of seizures.129 Rasmussen and Penfield found that stimulation of the precentral gyrus immediately anterior to the central sulcus (area 8) resulted in contralateral eye deviation;107 less often ipsilateral deviation or upward deviation and convergence occurred. However, stimulation of more anterior sites always resulted in contraversion.117 Version may also occur upon stimulation of the occipital lobe.10,104,120,129 Version occurs on the same side as dystonic posturing68 and is usually but not always followed by a secondarily generalized tonic–clonic seizure.13,21,68,129 Version occurs in partial onset seizures originating from a number of different locations that spread to the premotor cortex. Chee et al. found that version occurred earlier than 18 seconds in extratemporal seizures and later than 18 seconds in the vast majority of temporal lobe seizures.21 This is, of course, due to more rapid spread to the prefrontal cortex in extratemporal seizures (the majority starting from the frontal lobe). Ipsilateral forced eye and head deviation occurs in frontal lobe seizures; later in the seizure, contralateral version occurs just prior to secondary generalization. Some authors reported forceful head turning occurring ipsilaterally to the focus;44,95,109 these could be due to (a) seizures beginning in the area where Penfield and Rasmussen found ipsiversive movements, (b) rapid contralateral spread to homotopic frontal eye fields, or (c) disruption of normal pathways due to structural lesions.16 In our experience, version occurring just prior to a secondary generalization has always been correct in lateralizing the side of ictal onset.13,21 At the end of the generalized convulsion, Wyllie et al. have noted ipsilateral head and eye deviation (ipsiversion), which is presumed to reflect activation of the opposite hemisphere and neuronal exhaustion on the side of seizure onset.130 Ictal SPECT scans in versive seizures show localized hyperperfusion in the region of the sensorimotor cortex.54,92,125 Asymmetric tonic limb posturing, sometimes referred to as the “Figure 4 sign,” occurs in the course of secondarily generalized tonic–clonic seizures, and is usually contralateral to the side of ictal onset.69
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


