♦ Preoperative
Operative Planning
- Review imaging (magnetic resonance imaging)
Routine Equipment
- Laminectomy instruments
- Microsurgical instruments
- High-speed drill (optional)
Special Equipment
- Consider neurophysiological monitoring of somatosensory evoked potentials and motor evoked potentials
Operating Room Set-up
- Open-frame spinal table or electric table with bolsters or Wilson frame
- Ensure ability to obtain anteroposterior and lateral radiographs to confirm operative levels
- Headlight
- Loupes (optional)
- Bipolar and Bovie cautery
- Microscope with bridge
Anesthetic Issues
- General anesthesia
- Arterial line for blood pressure monitoring
- Intravenous antibiotics (cefazolin 2 g or vancomycin 1 g for adults) should be given 30 minutes prior to incision
- Dexamethasone is given to reduce swelling
- Minimize halogenated inhalational agents and nitrous oxide if neurophysiological monitoring performed
♦ Intraoperative
Positioning
- Patient prone
- Secure head with foam mask, Gardner-Wells tongs with 15 lb of traction, or Mayfield head holder
- If using foam mask, ensure no ocular pressure
- For lesions at T6 or above, pad arms and tuck along sides; for more distal lesions, abduct shoulders and flex elbows 90 degrees
Sterile Scrub and Prep
- As for posterior cervical or posterior thoracic approach
Incision
- Center linear midline incision over the levels of the lesion to permit exposure of one level above and one level below the lesion
Laminectomy
- Bilateral subperiosteal exposure to medial facet joints bilaterally
- Perform bilateral laminectomies from one level proximal to one level distal to the cavernous malformation
- Do not violate facet joints (may lead to postoperative kyphotic deformity)
- Wax bone edges, obtain meticulous epidural
Dural Opening
- Open dura in midline
- Secure edges of dura to paraspinal muscles with 4–0 silk tacking sutures
Resection (Fig. 139.1)
- Identify location of lesion by inspection; the pia overlying the cavernous malformation may be identified by its grayish blue discoloration
- Intraoperative ultrasound may be helpful if lesion not visible on dorsal spinal cord
- Perform sagittal, linear myelotomy over the area of the lesion where it appears most superficial; for more deeply situated lesions, may retract the margins of the myelotomy with pial sutures
- Develop a plane between surrounding gliotic tissue and the lesion with a microdissector
- Cauterize lesion if necessary to shrink it and facilitate dissection
- Inside out piecemeal dissection of the lesion may minimize trauma to surrounding spinal cord
- If cavernous malformation is located ventrally, exposure may require division of the dentate ligaments to allow mobilization of the spinal cord
- May safely evacuate old hemorrhages
- Ensure complete resection
Closure
- Close dura primarily with 4–0 silk running suture, either locked or unlocked
- May use onlay dural substitute sealed with fibrin glue or similar product
- Place drain, if necessary, deep to fascia
< div class='tao-gold-member'>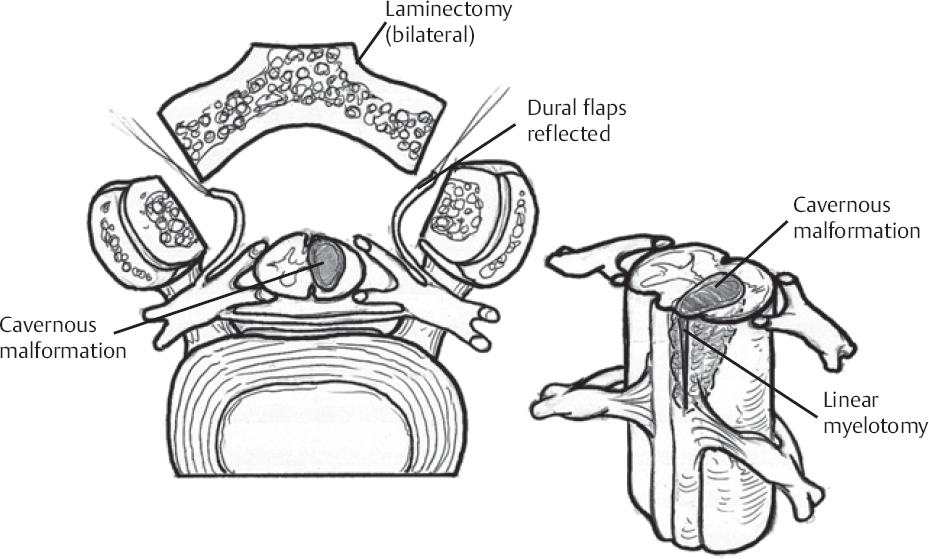 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


