Chapter 16 Spontaneous Intracerebral Hemorrhage
• Hemorrhagic stroke accounts for 10% of all strokes. Strokes are the third leading cause of death and the main cause of long-term disability in the United States.
• Spontaneous intracerebral hemorrhage (ICH) is most commonly caused by chronic hypertension and occurs in penetrating arteries in the basal ganglia, thalamus, pons, and cerebellum. However, other causes, such as vascular malformations, tumors, and amyloid angiopathy, should always be considered.
• The presentation of ICH depends on its location, with neurological deficits being specific to the function of the brain involved. A decreased level of consciousness can occur with large lesions that cause herniation or lesions in the posterior fossa that result in brainstem dysfunction or hydrocephalus.
• The prognosis for ICH depends on the location and size of the hemorrhage, the age of the patient, and the degree of neurological impairment at the time of presentation.
• Medical therapy can try to prevent expansion of the hematoma, but emergent surgical evacuation should be considered for patients with rapid deterioration.
Background and Epidemiology
Spontaneous intracerebral hemorrhage is defined as a nontraumatic hemorrhage into brain parenchyma. The clinical significance of intracerebral hemorrhage (ICH), also known as hemorrhagic stroke, can be more clearly understood when it is viewed as a subtype of stroke. According to the National Vital Statistics Report, stroke is the third leading cause of death in the United States, behind only heart disease and cancer, and is responsible for nearly 6% of total deaths on an annual basis.1 ICH accounts for approximately 10% of all strokes with an annual incidence between 15.9 and 32.9 per 100,000.2 A sharp increase in incidence occurs in patients more than 75 years old and the incidence is even higher in patients older than 85, with reported incidence rates as high as 309.8 per 100,000, nearly seven times greater than the rate in the general population.3 Though less frequent than ischemic stroke, the overall mortality rate of ICH is significantly greater, with 30-day mortality estimated at 44% to 52% and half of all deaths occurring within the first 2 days of hemorrhage.4–6 The national cost of first-time strokes has been estimated at $40.6 billion, with more than $6 billion accounting for aggregate lifetime cost.7 Of the $40.6 billion, only 45% of the cost was attributable to acute stroke care, with more than 47% of the total cost coming from long-term ambulatory and nursing care. Of all patients with ICH, only 20% have been noted to be functionally independent 6 months after their stroke.5 Although these statistics underscore the significant economic burden of ICH, they fail to emphasize the immeasurable emotional and social impact of ICH. It is essential to note, however, that since 1958, there has been a general annual decline in stroke deaths nationally. Between 2005 and 2006, there was a 6.4% decrease in stroke deaths.1 This decline is attributable to significant improvements in treatment of modifiable risk factors related to cardiovascular and cerebrovascular health. Still, the rate of ICH is expected to increase in the future as a result of increasing population age.
Pathophysiology
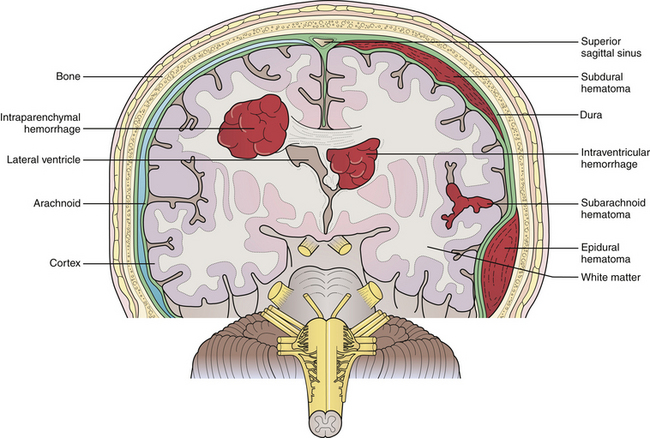
ICH may be classified as primary or secondary, depending on the etiology of the hemorrhage. Primary ICH most commonly results from chronic arterial hypertension. It occurs in small perforating arteries, typically at bifurcations from larger cerebral arteries where a pressure gradient is transmitted from the larger vessel to smaller, susceptible vessels. Small perforating vessels with diameters of 50 to 700 µm are often the offending vessels and may have multiple sites of rupture.8 Hypertension is the most important risk factor for ICH, with nearly 60% of patients with ICH in a prospective study having elevated blood pressure.9 Hypertensive bleeds are noted to occur more frequently within deep gray matter structures, most commonly the basal ganglia, followed by the thalamus, pons, and the cerebellum (Fig. 16.1). Lobar hemorrhages, however, are not infrequent. Of all ICHs, one population study reviewed the locations of cerebral bleeds and noted 49% were deep in location, 35% were lobar, 10% were in the cerebellum, and 6% were in the brainstem.10
Classically, hypertensive bleeds have been attributed to the rupture of miliary aneurysms as described initially by Charcot and Bouchard in 1868 from their postmortem analysis of hemorrhage cavities in autopsy specimens. Further research has clarified that the miliary aneurysms described by Charcot and Bouchard are in fact pseudoaneurysms or weaknesses in the perforating arteriole walls where there has been extravasated blood and accumulated fibrin.11 Pathological analysis of vessels in ICH specimens and in patients with chronic hypertension has more clearly demonstrated the process of lipohyalinosis in which chronic hypertensive damage gives rise to intimal hyperplasia, fibrin deposition, and focal accumulation of fat-filled macrophages, ultimately leading to necrosis in the vessel walls.11 These vessel changes are more commonly seen at sites of hemorrhages than miliary aneurysms and thus are believed to be the source.
After the inciting hemorrhage, blood disperses along surrounding fiber tracts in the parenchyma. In an estimated 10% to 15% of cases, blood will decompress from the parenchyma into the ventricular system, creating an intraventricular hemorrhage.12 Ultimately, the hemorrhage is self-contained by tamponade from the parenchyma adjacent to the bleed site and by activation of hemostatic pathways. Regions of brain surrounding a hemorrhage are often characterized by extensive inflammation, edema, apoptosis, and necrosis that may contribute to the neurological deficit. Moreover, increased intracranial pressure and herniation secondary to mass effect occur with particularly large-volume hemorrhages. The rate of expansion of a hemorrhagic lesion is also an important variable to consider. Rapidly expanding lesions cause greater direct injury to axons and tissues and therefore result in greater damage to adjacent neural structures than slowly expanding lesions.
Secondary ICH results from underlying lesions such as aneurysms, vascular malformations, coagulopathies, tumors, hemorrhagic conversion of ischemic infarcts, cerebral amyloid angiopathy, and drug-related hemorrhages. Common metastatic tumors that are prone to hemorrhage include melanoma, choriocarcinoma, and renal carcinoma. Lung and breast cancer should also be considered because of their high incidence in the population. Primary brain neoplasms associated with ICH include glioblastoma multiforme, oligodendroglioma, and ependymoma.13 Although secondary ICH is less common, it is important to consider these causes in the differential diagnosis and work them up appropriately because they place patients at risk for recurrent hemorrhage with the potential for extensive morbidity and even death.
Etiology
Hypertension
Normal blood pressure is currently defined as systolic blood pressure (SBP) less than 120 mm Hg and diastolic blood pressure (DBP) less than 80 mm Hg. Hypertension is currently classified as four stages: prehypertension (120-139/80-89 mm Hg), stage 1 hypertension (140-159/90-99 mm Hg), stage 2 hypertension (160-179/100-109 mm Hg), and stage 3 hypertension (≥190/≥110 mm Hg). Multiple studies have verified the dramatically increased risk of ICH as it corresponds to increases in hypertensive stage.9,14–16 One meta-analysis of 11 case-control studies reported an overall odds ratio of 3.68 for ICH in hypertensive patients. Relative risk for patients with high normal hypertension (130-139 mm Hg systolic or 85-89 mm Hg diastolic) was 2.2, 5.3 for stage 1 hypertension, 10.4 for stage 2 hypertension, and 33.3 for stage 3 hypertension, as described by Suh and colleagues.16 Individuals with stage 3 hypertension are five times more likely to experience ICH than individuals with normal blood pressure or prehypertension. The rate of ICH increases 22% for every 10 mm HG increment of SBP.9 Naturally, improvements in hypertensive management and available antihypertensive medications have aided in decreasing the incidence of intracerebral hemorrhage.17
Cerebral Amyloid Angiopathy
In the elderly population, cerebral amyloid angiopathy (CAA) is an important etiological factor for ICH, accounting for an estimated 5% to 10% of all cases.18 CAA results from the deposition of β-amyloid in the media and adventitia of cerebral vasculature, including capillaries, arterioles, and even small to medium-sized cerebral arteries in the cerebral cortex, leptomeninges, and cerebellum. CAA is commonly associated with the gene encoding apolipoprotein E, and a familial syndrome has been described accounting for CAA-related hemorrhages in younger patients.19 For every decade increase in age, there is a 1.97 relative risk increase for ICH and a three times and seven times increased incidence rate for patients aged 65 to 74 and greater than age 85, respectively.14,20 ICH due to CAA is most commonly in lobar locations, classically in the posterior parietal and occipital lobes. Special consideration of CAA should be given for bleeds in these locations, especially in elderly patients.12 Recurrent lobar hemorrhages are relatively common in CAA and account for substantial increases in morbidity and mortality rates. The 2-year recurrence rate of lobar hemorrhages in patients with known CAA is 28%.21
Anticoagulation Therapy
ICH is a common yet serious complication of anticoagulation therapy. Patients on oral anticoagulation therapy suffering from ICH typically have significant vasculopathy related to chronic hypertension or CAA.22 There is a 1% per year increase in risk for ICH while on anticoagulation therapy, seven to ten times the rate in the normal population.23 This increased risk is quite significant given the high mortality rate of ICH associated with anticoagulation therapy, which is approximately 70%.24 Moreover, patients on oral anticoagulation therapy have a significantly greater hematoma volume than patients not on anticoagulation. Prompt recognition of ICH is essential in this patient population, with particular attention paid to correcting the coagulopathy and stabilizing hematoma expansion.
Drugs and Alcohol
Certain drugs are capable of causing spontaneous ICH. Those most commonly associated with ICH are sympathomimetic agents, such amphetamines, cocaine, and pseudoephedrine. Hemorrhages associated with sympathomimetic agents are often related to transient elevations in blood pressure, leading to arterial rupture. Additionally, transient hypertensive episodes associated with substance abuse may cause hemorrhage from an otherwise asymptomatic vascular lesion such as an aneurysm or arteriovenous malformation. In younger age groups, cocaine abuse is commonly associated with ICH and subarachnoid hemorrhage.25 As such, underlying vascular pathology should still be considered in young patients with ICH.
ICH has also been associated with alcohol consumption. Juvela and colleagues demonstrated an increased risk of ICH in patients who were moderate or heavy drinkers in a dose-dependent manner. A positive CAGE questionnaire∗ was associated with increased risk of ICH.26 The exact pathophysiological mechanism by which alcohol contributes to ICH is not clear; however, alcohol-associated hypertension, impaired hemostasis, and decreased levels of clotting factors have been implicated.
Aneurysms
Saccular Aneurysms
The majority of aneurysms are saccular aneurysms whose etiology may be a combination of congenital, hereditary, and acquired factors, including smoking and hypertension. The mortality associated with subarachnoid hemorrhage from a saccular aneurysm rupture is estimated to be between 40% and 50%, making this a grave disease.27
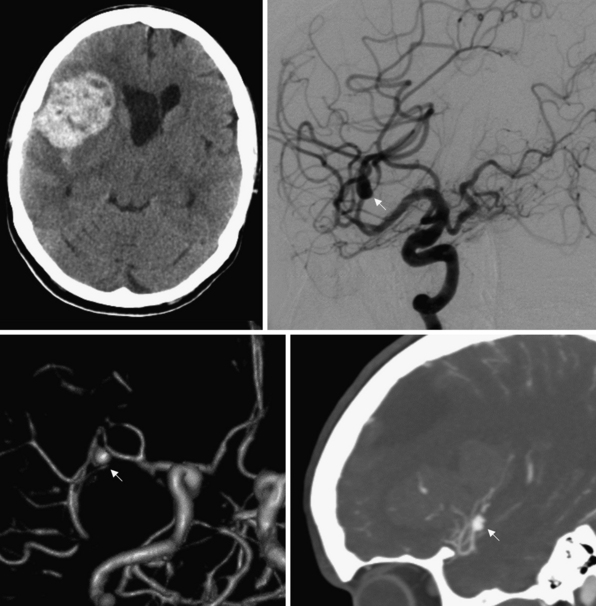
Saccular aneurysms are typically located at branch points of major cerebral arteries, usually arising from the vessels that form the circle of Willis. Saccular aneurysms may be associated with inherited conditions, including Ehlers-Danlos syndrome, adult polycystic kidney disease, and other conditions that predispose individuals to aneurysm formation because of intrinsic weaknesses in their vessel walls. In fact, 20% of patients with saccular aneurysms harbor more than just one. Additionally, lesions that alter cerebral blood flow, such as tumors or vascular malformations, may lead to aneurysm formation. Bifurcations and trifurcations are particularly susceptible areas for aneurysm formation because these points experience a greater hydrostatic pressure owing to loss of laminar blood flow and greater turbulence. Although saccular aneurysm rupture usually leads to subarachnoid hemorrhage, intraparenchymal hematomas into adjacent brain are common (Fig. 16.2). The presence of an intraparenchymal hematoma after aneurysm rupture may play an important role in the need for and timing of surgical intervention.
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


