Epileptic seizures are paroxysmal events, and many, if not most, are likely precipitated by known or unknown factors acting on a central nervous system (CNS) that is predisposed to the production of epileptic discharges by the presence of an organic lesion, a genetically determined neuronal hyperexcitability, or both. The known precipitating influences are quite varied. Aird (1988) indicated that 40 seizure-precipitating mechanisms are known, some 10 of which vary from hour to hour depending on habits and the daily activities of the patients. Tension states, alterations in the level of consciousness, sleep deprivation, disturbances of acid-base and water balances, drug withdrawal, proconvulsant drugs, and sensory stimuli all are important factors. Psychologic factors are probably common precipitants of certain types of seizures (Wolf and Inoue, 2002; Verduyn et al., 1988). Some may be specific, with a given psychologic situation regularly provoking seizures. More commonly, seizure-facilitating psychologic factors are nonspecific; these may include stress (Friis, 1990; Aird, 1988); excitation; or, conversely, inattentiveness and boredom (Papini et al., 1984). The regulation of such precipitating factors, both psychologic and otherwise, may play a significant role in the stabilization and improvement of epilepsy in selected patients. One estimation has indicated that such factors were of crucial importance in 17% of a group of refractory patients (Aird et al., 1984).
In some cases, specific stimuli regularly and reproducibly evoke seizures or facilitate their occurrence (Newmarck, 1983). These stimuli are of various natures, and some (e.g., hyperventilation) are routinely employed in the diagnosis of some forms of epilepsy (see Chapter 8). Seizures induced by specific sensory stimuli, which are often called reflex epilepsy (Zifkin et al., 1998), and, to a lesser extent, by specific psychic precipitants form a small but interesting set of seizure disorders. Such seizures may be broadly classified into two groups. The first group includes those patients in whom attacks are always or almost always evoked by a specific stimulus, such as flickering light, reading, and music. The second group consists of those who have spontaneous seizures in addition to their stimulus-sensitive attacks. The second type is relatively common, and 5% to 6% of patients with epilepsy are estimated to have a seizure disorder that some specific sensory stimuli may exacerbate (Binnie and Jeavons, 1992). Such a distinction, however, is not absolute because the epilepsies of some patients may pass through successive stages during which seizures occur spontaneously or only after exposure to a specific stimulus. Stimulus-sensitive seizures are often clinically stereotyped, and they are associated with a consistent electroencephalographic (EEG) pattern that may be reproduced under laboratory conditions. However, the appearance of a well-defined EEG pattern with exposure to a given stimulus is not sufficient to characterize the associated seizures as “stimulus sensitive.” Many patients, for example, exhibit a photoparoxysmal EEG response, although their actual seizures are not precipitated by light. This chapter considers only those cases in which specific stimuli are associated with clinical seizures, whether they are always precipitated by the specific stimulus or are associated with spontaneous seizures, not those in which stimuli evoke only an EEG response. Situation-related epilepsies, which are considered elsewhere in this book (see Chapter 15), differ from true stimulus-sensitive epilepsies by their mechanisms and mode of provocation because the seizures preferentially occur in specific circumstances.
Although some stimuli are closely associated with certain types of seizures (e.g., reading with jaw jerks or photic stimulation with generalized myoclonic jerks), no strong correlation between any one stimulus and a specific type of attack has been found, and the same stimulus may be effective in quite different clinical contexts. For example, photic stimulation can produce attacks in patients with structural brain lesions or metabolic disorders, as well as in those with idiopathic epilepsy.
In children and adolescents, visually evoked seizures are, by far, the predominant form of stimulus-sensitive epilepsy. Startle epilepsy is also relatively common; other stimuli only rarely provoke seizures.
PHOTOSENSITIVE EPILEPSIES AND OTHER EPILEPSIES RELATED TO THE VISUAL SYSTEM
Photosensitivity, also known as visual sensitivity, may be defined as an abnormal EEG or clinical response to flickering light (Kasteleijn-Nolst Trenité et al., 2001; Newmark and Penry, 1979). The purpose of this section is not a study of photosensitivity, which is essentially a laboratory finding established only by the use of an appropriate technique. Excellent reviews of this topic are available elsewhere, and they include discussions of the many necessary factors for light stimulation to be effective in the laboratory (Takahashi, 2002; Kasteleijn-Nolst Trenité et al., 2001; Guerrini et al., 1998d; Harding and Jeavons, 1994; Wilkins and Lindsay, 1985). The greatest clinical significance is attached to the photoparoxysmal response, also termed photoconvulsive. This is a paroxysmal; focal; or, most often, generalized discharge of spike-waves, polyspike-waves, or occasionally multiple spikes that is elicited by photic stimulation. Although the traditional belief was that epilepsy was more common if the photoparoxysmal response was continued for 100 ms or longer after the stimulus ends (Reilly and Peters, 1973), this has not been confirmed in more recent studies (Jayakar and Chiappa, 1990). The photoparoxysmal response should be separated from the photomyoclonic response, which is anteriorly located and is always associated with myoclonic jerks of the periocular muscles and muscles of the face that are time-locked to the flashes of intermittent photic stimulation (IPS) and are sometimes accompanied by vertical oscillations of the eyeballs (Kasteleijn-Nolst Trenité et al., 2001). The photomyoclonic response is blocked by eye opening, and it stops immediately after the stimulation is terminated. The frequency range of the flashes that is effective in triggering the photomyoclonic response is usually between 8 and 20 Hz. The photomyoclonic response is rarely seen in children. The current understanding indicates that it is an expression of cortical response within the spectrum of photic cortical reflex myoclonus (Artieda and Obeso, 1993).
Photosensitive epilepsies are characterized by the occurrence of seizures evoked by photic stimuli that occur under everyday environmental circumstances; these can be divided into two broad categories (Kasteleijn-Nolst Trenité et al., 2001; Harding and Jeavons, 1994; Wilkins and Lindsay, 1985; Newmark and Penry, 1979; Forster, 1977). The first category includes those patients who have seizures only in response to flickering lights that they encounter in a normal environment. The second includes those patients who have spontaneous seizures in addition to attacks evoked by flickering light. In both categories, self-induction of seizures may occur, but it is much more common in the first. Such patients belong to different categories.
Categories of Photosensitive Epilepsies
The first category includes patients with a photoparoxysmal response in the EEG and no history of epileptic seizures. A photoparoxysmal response has been estimated to occur in about 4% of normal children or adolescents (Eeg-Olofsson et al., 1971). In such individuals, the abnormal EEG response to photic stimulation is usually detected by chance during an EEG that is performed for reasons unrelated to epilepsy. The likelihood of these children for developing epilepsy is unknown, but it has been estimated as roughly 20% in young adults (Kasteleijn-Nolst Trenité et al., 2001). Higher rates are highly likely in children as the reaction to IPS may increase during adolescence, leading to clinical seizures (Kasteleijn-Nolst Trenité et al., 1994).
Patients with spontaneous seizures only, but a photoparoxysmal response in the EEG may belong to various epilepsy syndromes.
A photoparoxysmal EEG response can be observed in patients with various epilepsy syndromes that are characterized by spontaneous seizures (Table 17.1). In many such patients, no evidence indicates that, in addition to the spontaneous seizures, photic-induced attacks also occur.
Patients in whom an isolated visually induced seizure, with or without a photoparoxysmal response in the EEG, occurs are not uncommon, especially in young adolescents in whom a single seizure may occur in front of the television, while playing with video games, or in a dance club. Generalized tonic-clonic seizures or prolonged visual seizures that may or may not be followed by unresponsiveness and secondary generalization may occur (Hennessy and Binnie, 2000; Guerrini et al., 1994, 1997a). Although a visual trigger is highly probable when ictal visual symptoms are present, the absence of a photoparoxysmal response is not uncommon even in such circumstances (Ferrie et al., 1994).
Patients with only recurrent visually induced seizures, with or without a photoparoxysmal response in the EEG, often have generalized tonic-clonic seizures or myoclonic jerks (Fig. 17.1). Some may present with focal occipital seizures with prominent visual symptoms, with or without secondary generalization (Hennessy and Binnie, 2000; Guerrini et al., 1995). In some children, seizures are observed only during IPS in the EEG laboratory. Such seizures rarely are generalized tonic-clonic convulsions, partly because the IPS is stopped when a photoparoxysmal response lasts too long (Binnie and Jeavons, 1992). Jeavons and Harding (1975) reported children in whom absences were regularly induced by IPS. The absences were evoked by a narrow range of frequencies (usually less than 15 per second). The average age at onset in the affected patients, two-thirds of whom were girls, was 12 years, which considerably exceeds the average age of patients with usual absence seizures (see Chapter 8).
TABLE 17.1.Epileptic syndromen with visual sensitivity
Generalized epilepsies
IGE, in order of age:
Benign myoclonic epilepsy of infancy (included late and reflex variants)
Childhood absence epilepsy
Juvenile absence epilepsy
Juvenile myoclonic epilepsy
GTCS on awakening
IGE with practice-induced seizures, including primary reading epilepsy
Visual sensitive IGE, including eyelid myoclonus with absences
Cryptogenic generalized epilepsies: epilepsy with myoclonic astatic seizures
Patients with visually induced and spontaneous seizures, with or without a photoparoxysmal response in the EEG, may belong to different syndromes.
Pattern Sensitivity
Overview
The precipitation of seizures by visual patterns is commonly associated with photosensitivity. Viewing linear patterns evokes epileptiform discharges in 30% of photosensitive patients if the pattern is static and in 70% if the patterns oscillate in a direction orthogonal to the line orientation (Wilkins et al., 1979b). The presentation of patterns is seldom effective in individuals who do not demonstrate a photoparoxysmal EEG response to IPS (Binnie and Wilkins, 1997). Those patterns that have been reported to induce epileptic attacks generally are strongly contrasting and black and white (Stefansson et al., 1977), but the character of inducing patterns can be quite variable. The occurrence of paroxysmal EEG activity in pattern-sensitive patients depends on the spatial frequency, orientation, contrast, and size of the pattern (Wilkins et al., 1979b; Porciatti et al., 2000). Oscillating and phase reversal patterns are more epileptogenic than drifting or static patterns (Wilkins et al., 1979b; Binnie et al., 1985b). The physiologic abnormality underlying sensitivity to both IPS and pattern stimulation appears to be the inability of the visual cortex to process afferent inputs of high luminance contrast through the normal mechanisms of cortical gain control (Porciatti et al., 2000).
Striped tissues, escalator gratings, radiators, and rugs have been incriminated in precipitating attacks in these patients. The induced seizures are usually tonic-clonic attacks, but absence seizures, myoclonic attacks, and partial seizures also occur (Dravet et al., 2002; Guerrini et al., 1995; Binnie and Jeavons, 1992; Newmark, 1983). Pattern-induced seizures are associated with sensitivity to flickering light in 70% to 100% of patients (Newmark and Penry, 1979; Stefansson et al., 1977). Adding a pattern to the lamps used for photostimulation may render them more effective in attack induction (Jeavons and Harding, 1975); however, only 2% of the patients of Jeavons and Harding (1975) had a history of pattern sensitivity, probably indicating that the effect of patterns may go unrecognized. Indeed, Binnie and Jeavons (1992) found that almost 20% of photosensitive patients reported precipitation by visual patterns when they were carefully questioned.
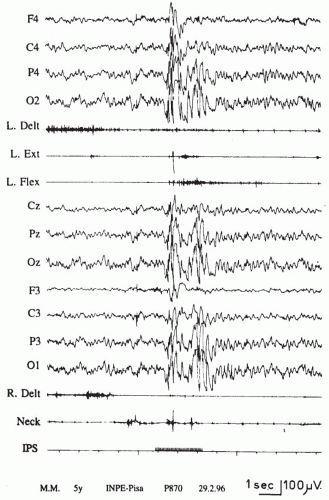
FIG. 17.1. Intermittent photic stimulation-induced generalized myoclonic jerks in a 5-year-old boy with myoclonic astatic epilepsy. A referential montage and a polygraphic recording are shown. Clinically, the child nods and briskly abducts his arms. The electroencephalogram shows a discharge of multiple spike-wave complexes that are generalized but that predominate posteriorly. Electromyographic myoclonic potentials are seen better on the wrist extensors and on the neck muscles.
The prevalence of photosensitive epilepsy in the general population is unknown. In an EEG study of 223 normal school children from 12 to 16 years of age of which only the boys were chosen to avoid the possible influences of hormonal variations, 3 children (1.3%) showed a generalized photoparoxysmal response. None had a clear history of seizures. Jeavons and Harding (1975) found 181 patients with seizures that were induced only by flickering light, 151 in whom spontaneous seizures also existed, and 122 patients who had a photoparoxysmal response without light-induced seizures. Dreifuss and Seino (Dreifuss, 1985) found 16 patients with attacks induced by environmental flickering lights, 31 with seizures induced by IPS in the laboratory, and 158 with a photoconvulsive response but not light-induced seizures. However, the patients in these studies were selected for EEG examination on the basis of clinical findings as mentioned earlier, studies in an unselected pediatric population show a photoparoxysmal response in 4% of individuals (Eeg-Olofsson et al., 1971). Binnie and Jeavons (1992) mention that the incidence of photosensitive epilepsy is roughly 1 in 4,000. In Western countries, the most common precipitant is television (Kasteleijn-Nolst Trenité et al., 2002b; Jeavons and Harding, 1975), which was reported to cause seizures in 299 of 461 patients of Jeavons and Harding (1975). Other investigators have reported lower figures (Binnie and Jeavons, 1992; Mayr et al., 1987). Although these discrepancies may reflect different criteria (e.g., Jeavons and Harding [1975] included patients with single attacks and a photoconvulsive response) (Newmark, 1983), the role of television in inducing these attacks is related to both its diffusion and to the characteristic screen frequency (50-Hz main screen frequency in Europe; 60-Hz main screen frequency in the United States and in part of Japan) (Kasteleijn-Nolst Trenité et al., 2001; Enoki et al., 1998; Harding and Jeavons, 1994). An outbreak of visually induced seizures was recently reported in Japan, where about 700 children and adolescents experienced photic-induced seizures while they were watching television broadcasting of a popular cartoon containing a scene with highly contrasting red-blue frames at 12 Hz (Harding, 1998; Takahashi and Tsukahara, 1998). Often children experience their first television-induced seizure while they are changing channels or are watching faulty channels, especially if they are close to the screen (Ricci et al., 1998). These children often use television for self-induction.
Computer screens may also cause photic-induced seizures. Their effectiveness as triggers is higher when they have a screen refresh rate of less than 70 Hz (Badinand-Hubert et al., 1998), especially when they are used for playing video games featuring highly contrasted, high-frequency stimuli (Kasteleijn-Nolst Trenité et al., 2002b; Ricci et al., 1998). Arcade video games have also been incriminated (Ferrie et al., 1994; Graf et al., 1994; Maeda et al., 1990). Some video games have been proven to be more provocative than standard television programs are (Kasteleijn-Nolst Trenité et al., 2002b). However, their efficacy in provoking seizures appears to be related to some specific features, including a bright background and flashing images. In addition, as has been observed with TV programs, playing the games on a 50-Hz television is significantly more provocative than is playing them on the 100-Hz television (Kasteleijn-Nolst Trenité et al., 2002b). Fatigue and stress have also been demonstrated to be cofactors in seizures precipitated during video game playing (Ferrie et al., 1994), but their role is difficult to demonstrate. Video game watching can also be provocative, although it is possibly less provocative than actually playing (Kasteleijn-Nolst Trenité et al., 2002b). Discotheque lighting and flickering sunlight are less common precipitants.
A strong genetic component underlies the photoparoxysmal response. Both dominant and multifactorial inheritance have been suggested by family studies (Doose et al., 1969; Davidson and Watson, 1956); however, a dominant mechanism with agedependent, but not sex-dependent, penetrance seems most likely (Waltz and Stephani, 2000). A photoparoxysmal response is most likely in patients and relatives with spontaneous generalized epileptiform discharges, but this can also be seen in individuals with spontaneous focal seizures (Doose and Gerken, 1973). Patients with JME may present with a different type of photosensitivity trait that has a higher chance of photoparoxysmal response in relatives (Tsai et al., 1989).
Pure Photosensitive Epilepsies
Flickering light is the most common known trigger of epileptic seizures (Kasteleijn-Nolst Trenité et al., 2001; Zifkin et al., 1998; Newmark and Penry, 1979; Forster, 1977). Pure photosensitive epilepsy is found in 40% of photosensitive patients (Binnie and Jeavons, 1992), and this includes patients in whom seizures are provoked only by environmental flicker stimulation. Environmental stimuli include flickering sunlight, such as that occurring when one is traveling along an avenue of trees or past railings or riding in a car (not driving) along a tree-lined road, sunlight shining through the leaves of trees, the interruption of light by helicopter blades, the reflection of sunshine on snow or from ripples on water, cinema screens, and oscilloscopes. As was already mentioned, television is the predominant cause. Television-induced or video game-induced seizures do not seem to differ from the pure photosensitive seizures precipitated by other flickering lights. The age and gender of the patients are similar, as are the types of attacks and the EEG manifestations (Guerrini et al., 1998d; Jeavons and Harding, 1975). Precipitation of seizures by both television or video games and other flickering lights is common (Jeavons and Harding, 1975).