♦ Preoperative
Operative Planning
- Review imaging (computed tomography, magnetic resonance imaging, magnetic resonance angiography, and/or angiogram)
- Spinal drain
Equipment
- Major craniotomy tray
- Mayfield head holder
- High-speed drill
- Leyla bar and Greenberg retractors
- Frameless stereotaxic equipment
Operating Room Set-up
- Headlight
- Loupes
- Bipolar cautery and Bovie cautery
- Cavitron ultrasound aspirator (Integra)
- Microscope
- Spinal drain insertion
Anesthetic Issues
- Communicate degree of intracranial pressure elevation to anesthesiologist
- Arterial line blood pressure monitoring
- Hyperventilation to pCO2 25 to 30 mm Hg
- Intravenous (IV) antibiotics (cefazolin 2 g or vancomycin 1 g) 30 minutes prior to incision
- Dexamethasone 10 mg IV preoperatively
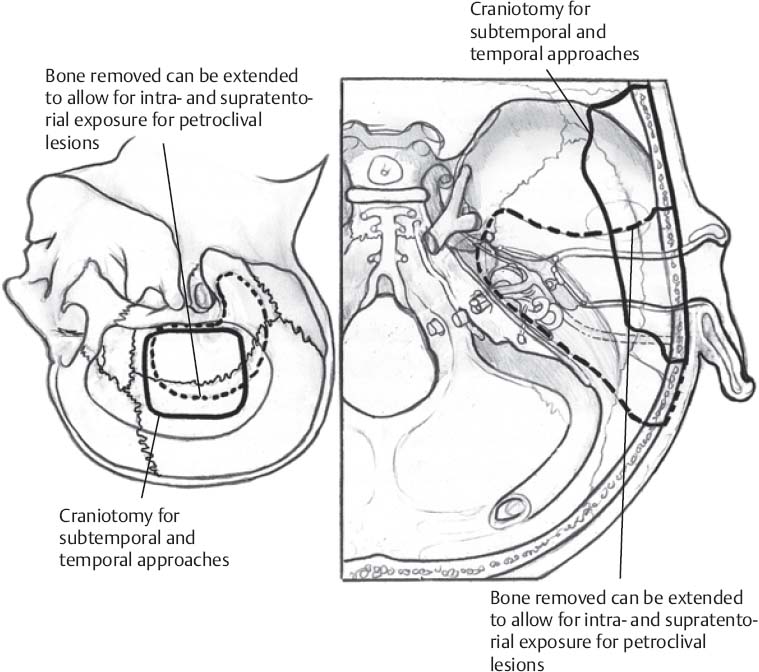
♦ Intraoperative (Fig. 11.1)
Positioning
- Patient supine with head turned 45 to 75 degrees toward the side opposite the lesion, with an ipsilateral shoulder roll
- Neck extended 15 degrees to lower the vertex and head elevated 20 degrees
- Heels and ulnar areas padded
- In patients with limited neck mobility, a full lateral position can be used, with the head elevated and the vertex lowered
- Minimal shave
- Use disposable razor
- Shave 2-cm wide strip along planned incision
- See Chapter 2, General Craniotomy Techniques
Subtemporal Approach
Incision
- A linear, 6-cm vertical incision is carried from the superior temporal line down over the zygoma 1 cm anterior to the tragus
- A self retaining retractor is placed
- The temporalis fascia is incised; the muscle is divided inline with the incision and dissected from the zygoma in the subperiosteal plane
Burr Hole
- A single burr hole is made in the squamous portion of the temporal bone immediately above the root of the zygoma
- The footplate attachment is used to strip the underlying dura from the bone
Craniotomy
- A temporal craniotomy is made with its inferior edge parallel and adjacent to the superior edge of the zygoma
- If necessary, additional bone is removed down to the floor of the middle fossa. Holes are drilled for tenting sutures.
- Surgicel is placed epidurally along craniotomy edges and epidural tenting sutures are placed
Dural Opening
- A T-shaped opening is made, with the vertical limb carried down to the middle fossa floor
- Dural tack up sutures are placed to the muscle
- Four sponges and towels are placed; the Greenberg retractor system is assembled
Temporal Lobe Elevation
- Two strips of Bicol (Codman) are placed over the anterior temporal lobe
- The temporal lobe is gradually elevated by advancement of the Bicol over the fusiform and then parahippocampal gyri, with Greenberg brain retractor blades and Cottonoids
- Small bridging veins can be divided to allow further temporal lobe retraction, but the vein of Labbe and large draining basal temporal veins should be preserved
- A subpial parahippocampal resection may be performed to widen the corridor to the lesion, when necessary
- Inferior retraction of the tentorium is accomplished by suturing the ten torial edge to the dura of the middle fossa, avoiding injury to cranial nerve (CN) IV
Subtemporal Transtentorial Approach
- A horseshoe skin incision is made starting from the zygoma 1 cm anterior to the tragus, extending above the pinna, and curving down ~2 cm behind the mastoid
- The scalp flap is reflected inferiorly down to the zygoma; care should be taken not to enter the external auditory canal
- Towel clips are placed at the base of the flap and secured to the Leyla bar with rubber bands for flap retraction
Burr Hole
- A single burr hole is made in the squamous portion of the temporal bone immediately above the root of the zygoma
Craniotomy
- A temporal craniotomy is made with its posterior extent just above the mastoid; additional bone is removed down to the middle fossa floor. The transverse sinus is freed and additional craniotomy is performed infratentorially if necessary.
- Mastoid air cells are generously waxed
- Holes are drilled for epidural tenting sutures
Extradural Dissection
- This is performed from a lateral to medial and posterior to anterior direction to avoid stretching the greater superficial petrosal nerve (GSPN) branch of the facial nerve.
- The following landmarks are identified:
- Tegmen tympani
- Arcuate eminence
- Lesser superficial petrosal nerve (LSPN)
- GSPN, middle meningeal artery
- Mandibular branch of the trigeminal nerve
- The LSPN can be distinguished from the GSPN because it joins the middle meningeal artery at the foramen spinosum
- Tegmen tympani
Dural Opening
- The dura is opened with a T-shaped incision along the inferior temporal lobe and with the vertical limb along the middle fossa floor
- Retraction of temporal lobe is performed with the aid of the operating microscope using the advancement of Bicol, Greenberg retractor blades, and Cottonoids, as in the standard subtemporal approach
- CN IV is identified; the division of the tentorium begins immediately posterior, a couple of millimeters off the petrous ridge
- The tentorial division is extended 3 to 4 cm posterolaterally and a couple of millimeters posterior to the superior petrosal sinus without injuring the sigmoid sinus. The division of the tentorium is carried in an anterolateral direction into the middle fossa and across the superior petrosal sinus with suture ligatures or titanium clips, resulting in an excised triangular flap of tentorium and a view down onto the clivus.
- Depending on the location of the lesion, additional bone removal of the posterior clinoids and/or petrous apex is performed if needed
Closure
- Dura closed with 4–0 silk sutures
- Central dural tenting sutures are placed and the dura is covered with dural substitute duraplasty (Duraform/Duragen)
- The bone flap is replaced and secured with titanium microplates
- The temporalis fascia is approximated with 2–0 Vicryl
- The galea is closed with inverted 3–0 Vicryl sutures
- The skin is closed with staples and Xeroform and head wrap applied
♦ Postoperative
- Steroid taper begins on postoperative day 1
- Antibiotics continued for 24 hours
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue








