♦ Preoperative
Operative Planning
- Review imaging: magnetic resonance imaging (MRI)
- Volumetric MRI with fiducials if frameless stereotaxy used for intraoperative guidance
Equipment
- Craniotomy tray
- Mayfield head holder
- High-speed drill
- Frameless stereotaxy
- Microscope (optional)
- Frameless stereotaxy (optional)
Operating Room Set-up
- Headlight
- Loupes
- Bipolar cautery and Bovie cautery
- Three-dimensional reconstructions and coregistrations performed if frameless stereotaxy used
- Micro scope
Anesthetic Issues
- Arterial line blood pressure monitoring
- Intravenous (IV) dexamethasone
- IV antibiotic prophylaxis
- Mannitol for brain relaxation
- Phenytoin load if not already maintained on anticonvulsants
♦ Intraoperative
Positioning
- Sitting slouch, lateral, or three-quarter prone with head in Mayfield three-point fixation
- Head is turned to side opposite lesion, vertex slightly elevated, and neck slightly flexed to allow as much of a straight, vertical approach to the parietal lesion as possible
- Ideally, head should be positioned so that a line drawn through the scalp entry point and the geometric center of the tumor is perpendicular to the floor
Minimal Shave
- Use disposable razor
Sterile Scrub and Prep
- See Chapter 2, General Craniotomy Techniques
Incision
- Depending on size of craniotomy, a linear (preferred) or a U-shaped incision based laterally can be used
Craniotomy
- Size and location of the craniotomy should be guided by frameless stereotaxy
- Single burr hole is usually sufficient
- Medial extent of bone flap should be at least 1 cm away from the midline to avoid the superior sagittal sinus and arachnoid granulations
- Bone flap elevated with Penfield no. 3 and flap elevator
- Holes for dural tenting sutures, central tacking suture, and microplate fixation of bone flap drilled, avoiding the medial edge near sagittal sinus
- Craniotomy edges lined with strips of Surgicel; 4–0 silk dural tenting sutures placed
Dural Opening
- Cruciate or U-shaped dural opening
- Moist “wall-off” cotton sponge is used to prevent drying of dural flap
- Corticectomy is started with pial cauterization using irrigating cautery, sharp division with pinch microscissors, and gentle suction to approach the lesion
- Lesion removal
- Two to four tapered retractors are advanced down to expose the surface of the lesion
- Microscope is useful to provide illumination as well as magnification
- Tumor internally debulked, allowing access to choroidal artery feeding the tumor (Fig. 8.1)
< div class='tao-gold-member'>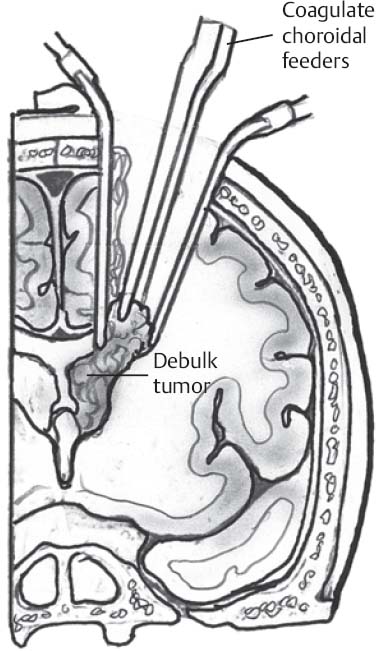
Fig. 8.1 Illustration of superior parietal approach. Debulking of tumor allows rotation to cauterize choroidal arteries.
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel
- Two to four tapered retractors are advanced down to expose the surface of the lesion






Full access? Get Clinical Tree


