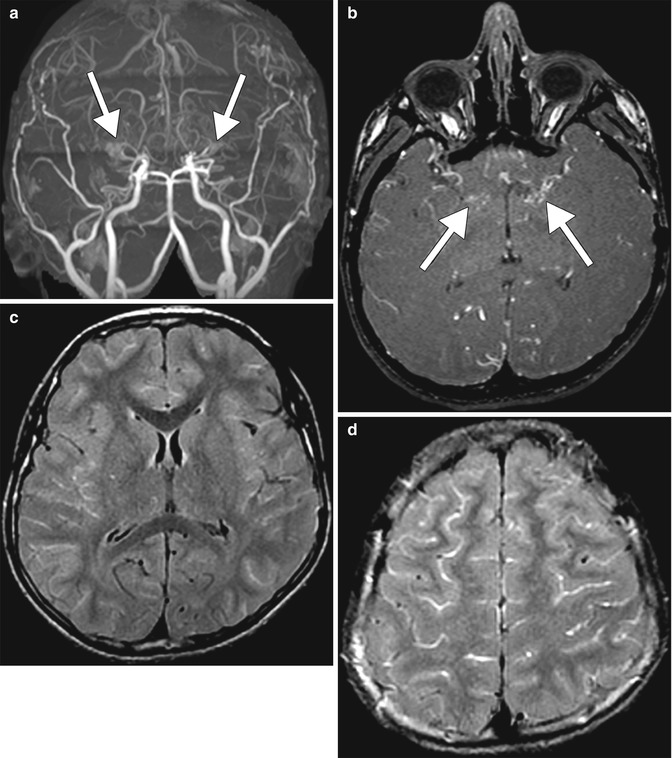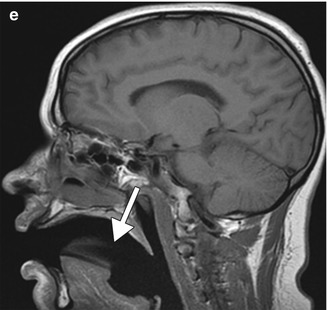
Fig. 35.1
Supplemental oxygen. Axial FLAIR MR images (a, b) show diffuse sulcal hyperintensity. The corresponding axial post-contrast T1-weighted (c) and susceptibility-weighted (d) MR images show no associated abnormal enhancement or evidence of blood products. Sagittal T1-weighted MRI (e) shows the presence of an airway mask (arrow)
35.4 Differential Diagnosis
Many conditions can produce the appearance of subarachnoid FLAIR hyperintensity, including subarachnoid hemorrhage, meningitis, sluggish blood flow in acute stroke, moyamoya, leptomeningeal carcinomatosis, leptomeningeal melanosis, delayed contrast leakage, CSF and vascular pulsation artifact, metal susceptibility artifact, and motion artifact. Some of these conditions are discussed and illustrated below:
Subarachnoid hemorrhage: High protein content and the diamagnetic properties of oxyhemoglobin in acute subarachnoid hemorrhage result in FLAIR hyperintensity. FLAIR is more sensitive than CT for the detection of acute subarachnoid hemorrhage (refer to Chap. 4). Susceptibility effect may also be present.
Meningitis: The presence of increased CSF cellular and protein content in inflammatory meningitis alters the CSF nulling point on FLAIR (Fig. 35.2). There may also be prominent leptomeningeal enhancement as well as associated cerebritis, abscess, and empyema.
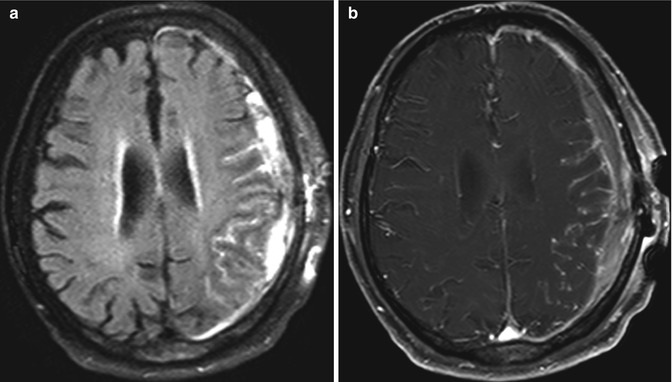
Fig. 35.2
Meningoencephalitis. Axial FLAIR (a) and axial post-contrast T1-weighted (b) MR images show sulcal FLAIR hyperintensity and enhancement, as well as cortical swelling in the left cerebral hemisphere
Cerebral ischemia: Vascular hyperintensity in the subarachnoid space on FLAIR results from severe stenosis or occlusion of major cerebral vessels, including moyamoya with slow pial blood flow that results in the “ivy sign” on FLAIR images (Fig. 35.3).