♦ Preoperative
Operative Planning
- Review imaging (magnetic resonance imaging preferred)
- Magnetic resonance angiography or angiography helpful for venous anatomy
- Avoid increased intracranial pressure (ICP) at surgery; consider ventriculos-tomy or ventricular drain for hydrocephalus, or preoperative third ventriculostomy if indicated
- If significant lateral or supratentorial component, may need other approach
- If lesion displaces deep cerebral venous complex inferiorly, may need supratentorial approach
- Lesions extending inferiorly or arising in the quadrigeminal plate may require an occipital-transtentorial approach
Equipment
- Major craniotomy tray
- Long bayonet “pineal” instruments
- Mayfield head holder
- High-speed drill
- Yasargil bar and Greenberg retractors
- Armrest
Operating Room Set-up
- Headlight
- Loupes
- Bipolar cautery and Bovie cautery
- Microscope (variable focal length preferred)
Anesthetic Issues
- Precordial Doppler monitor and attention to end-tidal pCO2 to diagnose air embolism; central venous access to aspirate air if embolism occurs
- Communicate degree of ICP elevation to anesthesiologist
- Arterial line blood pressure monitoring
- Hyperventilation to pCO2 25 to 30 mm Hg
- Intravenous (IV) antibiotics (i.e., oxacillin 2 g or vancomycin 1 g for adults) should be given 30 minutes prior to incision
- Dexamethasone 10 mg IV preoperatively
- Hyperventilation to pCO2 25 to 30 mm Hg
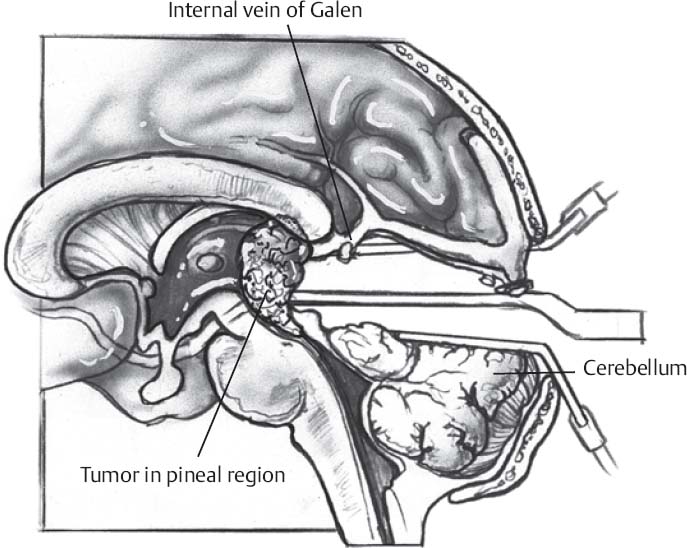
♦ Intraoperative (Fig. 16.1)
Positioning
- Patient in sitting position with trunk and neck flexed
- Head/neck flexed gently (maintain two fingerbreadths’ space between chin and sternum) so that tentorium is parallel to the floor
- Alternative: prone position
Minimal Shave
- Use disposable razor
- Three-cm wide strip shaved along planned incision
Sterile Scrub and Prep
- See Chapter 2, General Craniotomy Techniques
Only gold members can continue reading. Log In or Register to continue








