Chapter 39 Surgery for Trigeminal Neurinomas
Anatomy
The trigeminal nerve courses in three compartments: middle cranial fossa, posterior fossa, and extracranial space. Therefore, tumors extending into multiple fossae are common (58%)1 (Table 39-1). The most common origin is around the Gasserian ganglion (GG), showing a dumbbell-shaped tumor extending both middle and posterior fossae (MP type, 38.6%) through Meckel’s cave (MC). MC is a subarachnoid space depressed from the posterior fossa, separated from the cavernous sinus by a thin meningeal dura (dura propria), and opened freely to the posterior fossa containing loose trigeminal nerve bundles without perineural covering.2 However, the trigeminal nerves peripheral to the GG course in the interdural space, are wrapped with a so-called inner reticular layer (perineurium), and are easily separated from the lateral wall of the cavernous sinus by a cleavage plane3 (Fig. 39-1A).
Table 39-1 Location and Type of Tumor (MPE Classification)
| Tumor Type | Patients |
|---|---|
| M | 8 (14.0%) |
| P | 12 (21.1%) |
| E | 4 (7.0%) |
| MP | 22 (38.6%) |
| ME | 7 (12.3%) |
| MPE | 4 (7.0%) |
| Total patients | 57 (100.0%) |
| Compartment | |
| Single | 24 (47.3%) |
| Multiple | 33 (57.9%) |
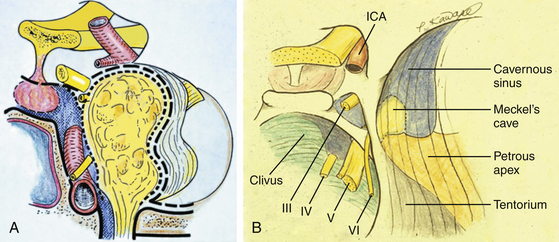
Therefore, the dumbbell-shaped tumor is spreading over the two anatomically different spaces: the interdural space anteriorly and the subarachnoid space posteriorly. The anterior part of the tumor can be removed through the interdural space by Dolenc’s approach.4 A small posterior fossa tumor can be removed through the orifice of MC; however, resection of the petrous apex, which obstructs the surgical field, is commonly necessary to observe the posterior fossa sufficiently. If the posterior fossa tumor is larger than 1 cm, the bone resection of the petrous apex plus detachment of the tentorium by the anterior petrosal approach (APA) is necessary.
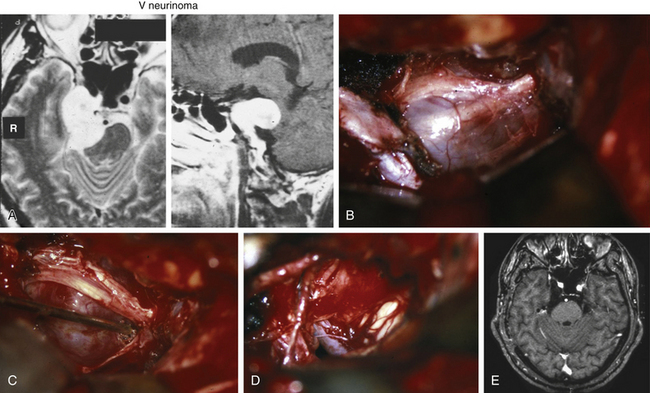
Resection of the petrous apex may offer a surgical effect to widen the surgical space, as well as to decrease the tension of the trigeminal bundle bent by the petrous apex (Fig. 39-1B). The posterior fossa (P) type of tumor commonly attaches on the trigeminal nerve bundle alone, and it can be removed by the APA,5 even when the tumor is large.
Selection of Surgical Approaches
• The subtemporal interdural approach (SIA) without zygomatic osteotomy is indicated for tumors of the middle fossa (M) or middle fossa and extracranial (ME) type (with infratemporal extension).
• The APA is indicated for MP-type (dumbbell-shaped) and P-type tumors.
• The zygomatic petrosal approach (ZPA), combining SIA and APA is indicated for large MP-type tumors or extension into three middle, posterior, and infratemporal fossae (MPE)–type tumors.
SIA WITH OR without Zygomatic Osteomy
The SIA is indicated for an M-type tumor with or without extracranial extension (Fig. 39-2). The zygomatic osteotomy is not always necessary but is effective to spare retraction damage to the temporal lobe by turnover of the temporal muscle inferiorly, especially for a large tumor extending higher than the tentorial fold. In the supine position, the patient’s head is rotated 60 degrees with a downward axis. A curved hemicoronal incision along the auricle is followed by exposure of the zygomatic arch, which is cut in two points by a surgical saw. The craniotomy is created along the middle fossa base to expose the foramen rotundum and ovale epidurally. The middle meningeal artery is coagulated and cut at the foramen spinosum. The periosteal side of the dura mater is incised above the foramen rotundum, and the incision is extended above the foramen ovale and toward the superior orbital fissure.
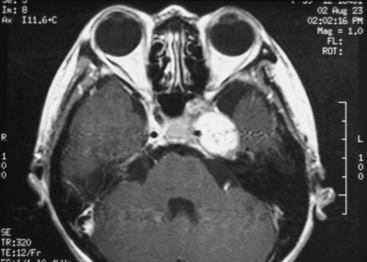
FIGURE 39-2 Parasellar type of trigeminal neurinoma. Note the compressed cavernous sinus medial to the tumor.
The lower part of the tumor appears by this point, and the upper part can be exposed by tacking the parasellar dura superiorly (Fig. 39-3). The tumor is commonly covered by a thin semitransparent membrane, the so-called inner reticular layer, showing the course of the trigeminal nerves through it (Fig. 39-3A and B).
< div class='tao-gold-member'>
Related posts:
 Chemotherapy for Brain Tumors
Current Surgical Management of High-Grade Gliomas
Endoscopic Endonasal Approach for Craniopharyngiomas
Revascularization Techniques in Pediatric Cerebrovascular Disorders
Surgical Management of Parasagittal and Convexity Meningiomas
Decompressive Craniectomy for Traumatic Brain Injury
Chemotherapy for Brain Tumors
Current Surgical Management of High-Grade Gliomas
Endoscopic Endonasal Approach for Craniopharyngiomas
Revascularization Techniques in Pediatric Cerebrovascular Disorders
Surgical Management of Parasagittal and Convexity Meningiomas
Decompressive Craniectomy for Traumatic Brain Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


