Chapter 68 Surgical Indications in Spine Trauma
Instability
As defined by White and Panjabi1 nearly two decades ago, instability is the inability “of the spine under physiological loads to limit patterns of displacement so as not to damage or irritate the spinal cord or nerve roots and, in addition, to prevent incapacitating deformity or pain caused by structural changes.” Their description of instability implies concepts of immediate or delayed neural compromise, deformity, and/or pain in conjunction with activities of normal daily living.
Determining spinal instability is not all black or white but, rather, encompasses shades of gray. Many schemes for the classification of instability have been suggested. In general, instability may be acute or chronic. Acute instability may be further defined as overt versus limited (Box 68-1). Acute instability may represent a threat to neural elements, may function as a pain generator, or may lead to progressive deformity if left unattended. Chronic instability may be subdivided as glacial instability, in which deformity occurs slowly over the course of time, similar to the movement of a glacier, or as a dysfunctional segment motion, in which the involved joint shows abnormal motion. As opposed to glacial instability, dysfunctional segment motion does not lead to deformity but rather to a pain syndrome associated with dysfunctional joint movement.
BOX 68-1 Instability Categorization Scheme
From Benzel EC: Biomechanics of spine stabilization, New York, 2001, Thieme.
Overt Instability
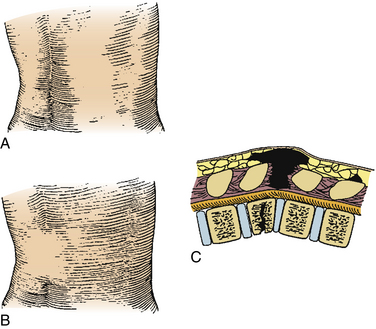
Overt instability is defined as the inability of the spine to support the weight of the torso. It is generally assumed when circumferential spinal integrity is lost. In effect, both anterior and posterior elements are compromised. Such injuries usually occur with larger force vectors or in patients with poor bone quality or biomechanical disadvantage (see later discussion). Compromise of the ventral elements can easily be demonstrated on plain film, CT, or MRI. Assessment of the dorsal elements, especially ligamentous structures, may be more challenging. Fat suppression or short tau inversion recovery (STIR) sequencing may illustrate ligamentous edema and suggest dorsal instability, but true disruption of the posterior tension band may be difficult to demonstrate.2 Flexion-extension films may be extremely dangerous in the face of overt instability. Disruption of the posterior ligamentous tension band may be noted on palpation of the affected area (Fig. 68-1).
Surgical Indications
Neural Compromise
Strong consideration should be given to patients with spinal cord, nerve root, and/or cauda equina compression with resulting neurologic deficits. Although still controversial, a growing body of evidence suggests that early decompression is the single most important predictor of neurologic recovery in spinal cord injury (SCI). Animal studies consistently show that neurologic recovery is enhanced by early spinal cord decompression.3,4 However, it is difficult to extrapolate the data for the effective application of decompression in the clinical setting from these animal models. To date, the clinical studies that have examined the role of surgical decompression in SCI are limited to class II and III evidence. One randomized controlled trial5 showed no benefit to early (<72 hours) decompression; however, several recent prospective series suggest that early decompression (<12 hours) can be performed safely and may improve neurologic outcomes.6,7 La Rosa et al.8 published a meta-analysis of the literature addressing the issue of early decompression and its role in acute SCI. They reviewed all published clinical studies and extracted data on 1687 patients. Patients were divided into three treatment groups: early decompression (<24 hours), delayed decompression (>24 hours), and conservative management. Statistically, early decompression resulted in better outcomes than either delayed decompression or conservative management. However, on homogeneity analysis, only data for patients with incomplete SCI who underwent early decompression were reliable. These studies concluded that early decompression can only be considered as a practice option. The Surgical Treatment of Acute Spinal Cord Injury Study (STASCIS)9 is a prospective, randomized controlled, multicenter trial that is currently in progress and seeks to determine the best timing of surgical decompression in SCI. In the authors’ opinion, surgery should be attempted in a medically stable patient as early as clinically feasible, often within 24 hours of admission.
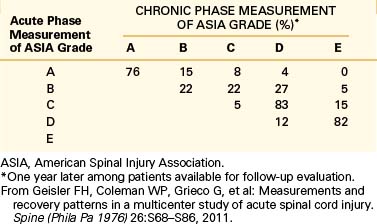
The American Spinal Injury Association impairment scale10 (ASIA), which is a modified Frankel classification,11 describes the completeness of an SCI. It has two main components: motor and sensory. The ASIA motor score of 0 to 5 is assigned for each muscle group innervated by spinal levels C5 to T1 and L2 to S1. This gives 10 levels on each side of the body, or a maximum possible score of 100. A sensory score of 0 to 2 is assigned for each dermatome from C2 to S4-5, using light touch and pinprick sensation. This gives 28 levels for a possible score of 56 on each side, or a maximum possible score of 112. Table 68-1 describes ASIA grading. The ASIA impairment scale has been shown to have great prognostic value, with chances of marked recovery more frequent in patients with better baseline scores. Table 68-2 shows the prognostic value of the ASIA impairment scale from the Sygen study group data.12
TABLE 68-1 American Spinal Injury Association Impairment Scale
| Class | Description |
|---|---|
| A | Complete: No motor or sensory function preserved in sacral segments S4-5 |
| B | Incomplete: Sensory but no motor function preserved below the neurologic level (includes sacral segments S4-5) |
| C | Incomplete: Motor function preserved below the neurologic level (more than half of key muscles below the neurologic level have a muscle grade <3) |
| D | Incomplete: Motor function preserved below the neurologic level (more than half of key muscles below the neurologic level have a muscle grade ~3) |
| E | Normal: Sensory and motor function normal |
From Frankel HL, Hancock DO, Hyslop G, et al: The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia 7:179–192, 1969.
Overt Instability
Columns
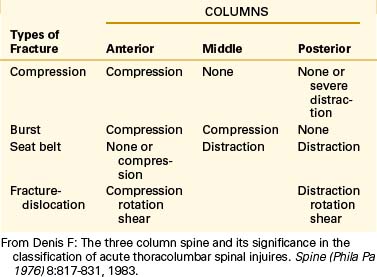
As previously described, overt instability refers to circumferential loss of spinal integrity. Compromise of only one column (either anterior or posterior) is considered limited instability only. The concept of “columns” is at the center of understanding spinal stability (Fig. 68-2) and dates back to the 1960s. In their seminal article, Kelly and Whitesides13 describe the concept of two columns as “one of solid bone and one composed of neural arches . . . Working together, these two columns support the body’s weight.” Later, Denis14 introduced the concept of a middle column, consisting of the posterior half of the vertebral body and disc and posterior longitudinal ligament. Depending on the pattern of column injury, he suggested four types of spinal fractures: compression, burst, seat belt–type, and fracture-dislocation (Table 68-3). The middle column suggested by Denis is interesting because it allows for specific assessment of the neutral axis. The neutral axis is the longitudinal axial weight-bearing zone about which spinal element distraction or compression does not significantly occur with flexion or extension (Fig. 68-3). As a rule, it is often suggested that compromise of two of the three Denis columns constitutes overt instability.

FIGURE 68-2 The “column” concepts of spinal stability. The concept described by Louis20 (left) assigns significance to the vertebral body and the facet joint complexes (lateral masses) on either side of the dorsal spine. Denis’s three-column concept (right) assigns significance to the region of the neutral axis and the integrity of the posterior vertebral body wall (the middle column). The two-column construct (left) relies on anatomically defined structures, the vertebral body (anterior column), and the posterior elements (posterior column). Louis’s three-column concept (left) similarly relies on anatomically defined structures.
(From Benzel EC: Biomechanics of spine surgery. Copyright © 2001 by the American Association of Neurological Surgeons, Rolling Meadows, IL.)
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


