♦ Preoperative
Operative Planning
- Review imaging
- Computed tomographic (CT) scan
- Location of fourth ventricular clot in the setting of subarachnoid hemorrhage, especially without supratentorial blood and blood primarily in the cerebellar pontine angle
- Degree of calcification in the setting of large and giant unruptured aneurysms
- Location of fourth ventricular clot in the setting of subarachnoid hemorrhage, especially without supratentorial blood and blood primarily in the cerebellar pontine angle
- Magnetic resonance image (MRI): helpful in identifying intraluminal thrombus in the setting of large and giant unruptured aneurysms
- Angiogram of PICA
- Relationship of the aneurysm to the origin of PICA: the aneurysm generally will have its neck at the origin of PICA but on occasion may involve PICA itself either alone or in addition to the vertebral artery
- Identify dominance of vertebrobasilar system: usually the aneurysm is on the dominant vertebral, but occasionally it may arise from the nondomi-nant vertebral or even vertebral ending PICA
- Relationship of the caudal loop of PICA to the foramen magnum when dealing with distal PICA aneurysms
- Nonsaccular aneurysms or wide-necked sessile aneurysms may often represent dissections and should be carefully reviewed because direct clip reconstruction is often more dangerous and no more efficacious than endovascular stenting or coiling
- Relationship of the aneurysm to the origin of PICA: the aneurysm generally will have its neck at the origin of PICA but on occasion may involve PICA itself either alone or in addition to the vertebral artery
- Angiogram of vertebrobasilar junction
- Note the rostral-caudal location of the vertebrobasilar junction: usually these aneurysms can be reached via a far lateral suboccipital approach; combined presigmoid–far lateral approach should be considered (with or without division of the nondominant sigmoid sinus depending on the projection of the aneurysm)
- Note the side of the confluens from which the neck of the aneurysm emanates: these lesions should always be approached from the side to which the aneurysm projects
- Note the rostral-caudal location of the vertebrobasilar junction: usually these aneurysms can be reached via a far lateral suboccipital approach; combined presigmoid–far lateral approach should be considered (with or without division of the nondominant sigmoid sinus depending on the projection of the aneurysm)
- Computed tomographic (CT) scan
- Coarse diamond drill bit for removal of the occipital condyle; alternative is the small matchstick (Midas Rex bit no. AM8)
- Fishhooks
- Micro-Doppler
- May need bypass tray, especially in case of distal PICA aneurysm where PICA sacrifice might be considered and in some cases may be augmented by PICA-PICA side-to-side anastomosis
- Radiolucent Mayfield head holder if intraoperative angiography
Operating Room Set-up
- As for acoustic neuroma
- A left-handed surgeon will have the nurse at the head for a right-sided approach with the assistant between them and the microscope base off to the surgeon’s right, next to the patient’s abdomen
- A right-handed surgeon will place the nurse to the right at the patient’s abdomen and the microscope stand at the patient’s head with the assistant in between
- A left-handed surgeon will have the nurse at the head for a right-sided approach with the assistant between them and the microscope base off to the surgeon’s right, next to the patient’s abdomen
Anesthetic Issues
- As for anterior communicating (ACOM) artery aneurysm
- Brain stem auditory evoked responses (BAERs) add little, and stimulation of the lower cranial nerves had not been a useful adjunct
♦ Intraoperative
Spinal Drain
- For subarachnoid hemorrhage (SAH) cases (regardless of the presence of ventricular drain)
- In the case of a poor dural closure, this drain may be left in for 24 hours to facilitate wound healing
Positioning
- For most patients, lateral position is best for easier exposure of bony midline and condyle
- Shoulder roll with the head turned may be reasonable alternative in some cases
- With either lateral or supine positioning flex the neck to open atlantooccipital space and increase light to operative field
- Head/shoulder should be above the heart
- Shoulder should be taped down with care to avoid upper trunk injury
Far Lateral Suboccipital Craniotomy
- As in Chapter 15, Far Lateral Approach
- Goal
- Early identification of the proximal vertebral artery
- Lateral to medial line of site
- Generous access to cerebellar hemisphere for retraction
- Early identification of the proximal vertebral artery
- Steps
- Curvilinear incision beginning over the cerebellar hemisphere and extending from the sigmoid-transverse junction medially to midline, leaving a dural cuff for closure and inferiorly to the arch of C2
- Spinal drainage and/or opening of the cisterna magna will relax the cerebellum
- Placement of dural tracking sutures sewn to the fishhooks to rotate the lateral dura maximally without compromising the sinus
- Curvilinear incision beginning over the cerebellar hemisphere and extending from the sigmoid-transverse junction medially to midline, leaving a dural cuff for closure and inferiorly to the arch of C2
Placement of Cerebellar Retractors
- Goal
- Proximal control
- Visualization of aneurysm
- Proximal control
- Steps
- Cover inflamed cerebellum with Surgicel; for unruptured aneurysms, this is not necessary
- Fitting of two retractors: one from above to lift tonsil (useful early in dissection), one from medial to retract flocculus (useful late in dissection)
- Use only one retractor at a time and give consideration to temporary vertebral artery occlusion and/or dissection of the clot from the cerebellum, to be retracted to prevent early rupture
- Cover inflamed cerebellum with Surgicel; for unruptured aneurysms, this is not necessary
Identification of Parent Vessel
- Goal
- Exposure of the aneurysm for clipping
- Steps
- Find vertebral artery as it enters the dura
- Prepare segment for temporary clip
- Find vertebral artery as it enters the dura
Identification of Aneurysm Neck
- Goal
- Exposure of the aneurysm for clipping (Fig. 25.1)
- Steps
- Find PICA and follow this to vertebral
- Stay on the vessel’s inferior surface during this dissection
- Find PICA and follow this to vertebral
Flow Arrest and Clipping
- Regardless of size, most PICA aneurysms benefit from clipping under flow arrest; this not only provides for vessel control in the event of intraoperative rupture but also lessens the turgor in the aneurysm, allowing for a milking action as the aneurysm is clipped; this enhances visualization and ensures noninclusion of the distal vertebral artery
- Clipping is usually accomplished with a straight clip; wide-necked aneurysms often involve a considerable portion of both the vertebral and the PICA, requiring a straight, fenestrated clip placed down the long axis of the vertebral; occasionally this may need to be backed up with a second clip
< div class='tao-gold-member'>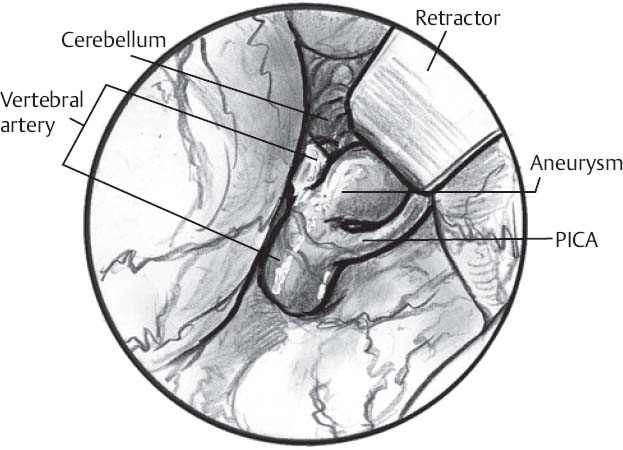 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continue








