♦ Preoperative
Operative Planning
- Obtain adequate imaging studies to rule out presence of an underlying mass lesion
- Magnetic resonance imaging (MRI) with and without gadolinium contrast
- Identification of the point where the syrinx is most superficial to the cord surface
- Shunt catheter should be placed in the most dependent portion of the syrinx, but above the level of injury in cases of traumatic syrinx
Equipment
- Major set-up
- Mayfield head clamp (for cervical or high thoracic cases)
- High-speed drill and Kerrison rongeurs
- Microinstrument set
- Silastic T-tube (Dow Corning, Midland, MI)
Operating Room Set-up
- Operating microscope with bridge attachment
- Monopolar and bipolar cautery
- Heparinized irrigating solution
- Dexamethasone
- Perioperative antibiotic coverage
- Somatosensory evoked potential and rectal-sphincter electromyography (optional)
♦ Intraoperative (Fig. 141.1)
Positioning
- Prone on the Jackson table or Allen table
- Alternatively, prone on a standard table with chest rolls and adequate padding to all pressure points
- Intraoperative imaging (x-ray or fluoroscopy) for localization prior to surgical site preparation
Planning of Incisions
- An approximate 15-cm midline incision centered on the level of interest
- Marking of the inferolateral rib cage in anticipation for possible syringopleural shunt
- Silastic T-tube removed and placed to soak in a bacitracin saline solution
Incision and Exposure
- Skin incised and paraspinal musculature is dissected along a subperiosteal plane with monopolar cautery
- Exposure and removal of the spinous process (by a Leksell rongeur) at the vertebral level of interest
- Laminectomy completed with high-speed drill or Kerrison rongeurs
- Exposure of the inferior aspect of the lamina above and the superior aspect of the lamina below
- Bone wax is applied to the bleeding bone edges for hemostasis
- Bipolar cautery utilized for control of any epidural bleeding
- Gelfoam soaked in thrombin is placed into the lateral epidural gutters
- Skin and surrounding area is covered with sterile towels
- Dura is elevated with a 4–0 Nurolon suture and incised with a no. 11 blade scalpel, leaving the arachnoid intact
- A dental instrument is placed into the subdural space, and the dural opening is extended in a rostrocaudal direction.
- Approximately 3 mm of dura is left unopened at the superior and inferior poles to facilitate dual closure at completion of the procedure.
- Dural edges are tacked to the paraspinal musculature with 4–0 Nurolon sutures
- Inspection of cord to identify most thinned portion followed by identification of the dorsal root entry zone
- Arachnoid is opened in a paramedian location and tacked to the dura with a 4–0 Nurolon suture
- Subarachnoid space is examined to identify any scaring and adhesions
- If significant adhesions are present, then a syringe-subarachnoid shunt is likely to fail, therefore a syringopleural or syringoperitoneal shunt should be performed.
< div class='tao-gold-member'>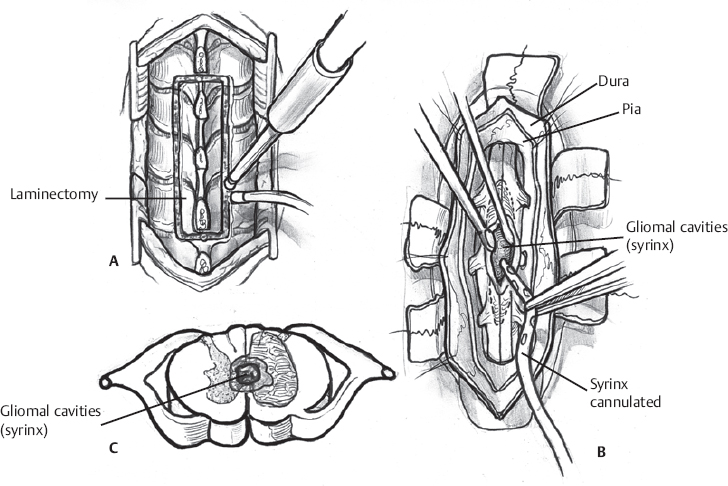 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


