T1 Isointense Suprasellar Mass
Anne G. Osborn, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Pituitary Macroadenoma
Pituitary Hyperplasia
Meningioma
Pilocytic Astrocytoma
Diffuse Astrocytoma, Low Grade
Less Common
Rathke Cleft Cyst
Germinoma
Neurosarcoid
Langerhans Cell Histiocytosis
Tuber Cinereum Hamartoma
Lymphocytic Hypophysitis
Rare but Important
Metastasis (Pituitary &/or Stalk)
Pituicytoma
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Where does lesion arise from?
Pituitary gland/sella turcica (macroadenoma, hyperplasia, hypophysitis, metastasis)
Infundibulum (germinoma, histiocytosis, pituicytoma)
Brain (astrocytoma), meninges (meningioma)
Does it enhance?
Yes: Macroadenoma, meningioma, aneurysm, neoplasm
No: Tuber cinereum hamartoma, RCC
Few lesions remain isointense with cortex on all MR sequences
Pituitary macroadenoma or hyperplasia
Meningioma, tuber cinereum hamartoma
Histiocytosis, sarcoidosis
Helpful Clues for Common Diagnoses
Pituitary Macroadenoma, Hyperplasia
Both isointense to gray matter (GM)
Meningioma
Usually isointense on all sequences
± Ca++, enhances
Astrocytomas (pilocytic > diffusely infiltrating)
Usually iso-/hypo- on T1, hyperintense on T2WI
Variable enhancement (none to striking)
Helpful Clues for Less Common Diagnoses
Rathke Cleft Cyst (depends on cyst content)
Most are hypointense
25% iso-, 10% hyperdense
Rim may enhance (“claw sign”)
Germinoma
Isointense on T1-, iso/hypo on T2WI
Enhances strongly, uniformly
Neurosarcoid, Langerhans Cell Histiocytosis
LCH (child), sarcoid (adult) → thick, enhancing stalk
Tuber Cinereum Hamartoma
> 90% isointense on T1WI, nonenhancing
May be slightly hyperintense on PD, FLAIR
Image Gallery
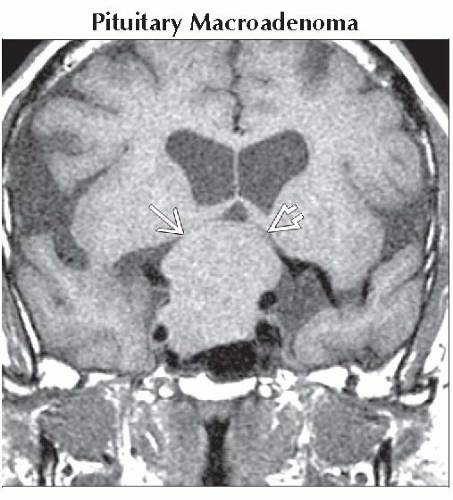 Coronal T1WI MR shows a large intra- and suprasellar mass
 elevating and compressing the optic chiasm elevating and compressing the optic chiasm  . The mass cannot be distinguished from the pituitary gland. . The mass cannot be distinguished from the pituitary gland.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|