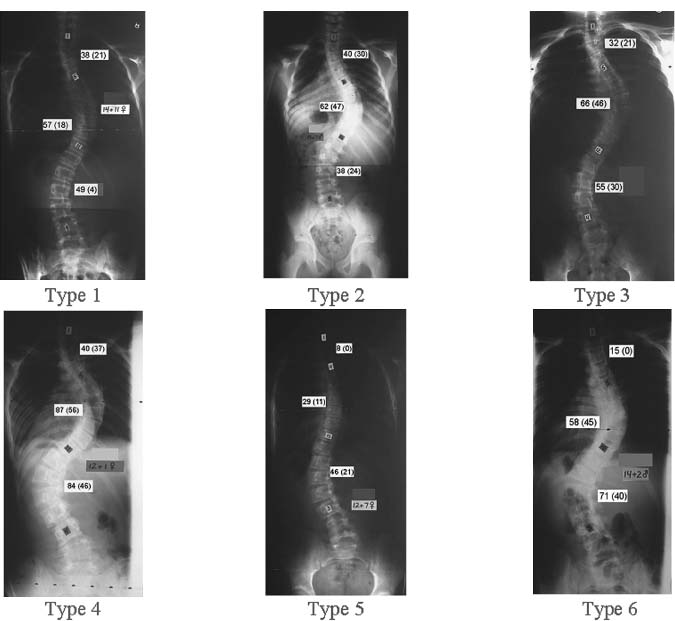
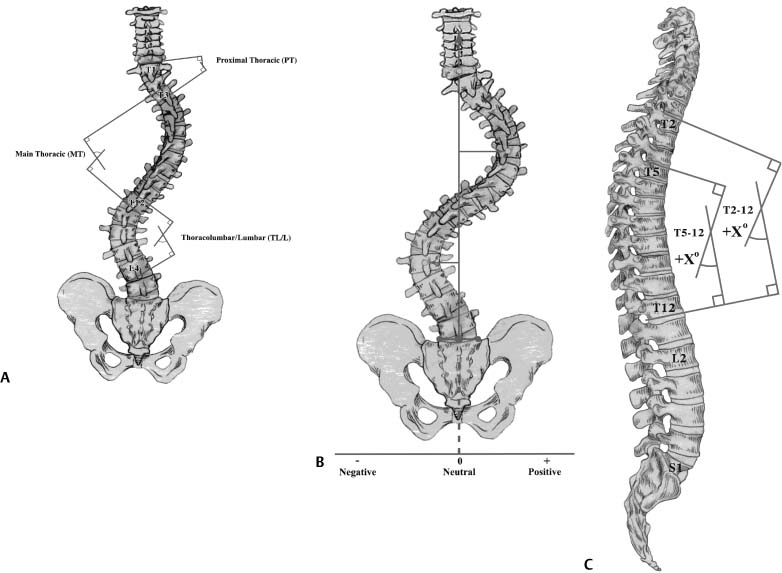
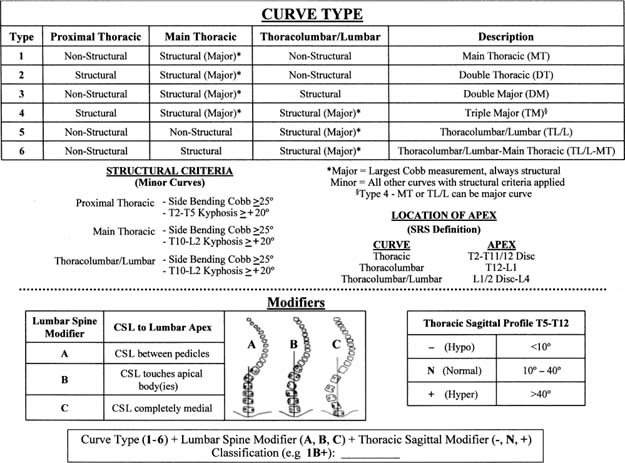
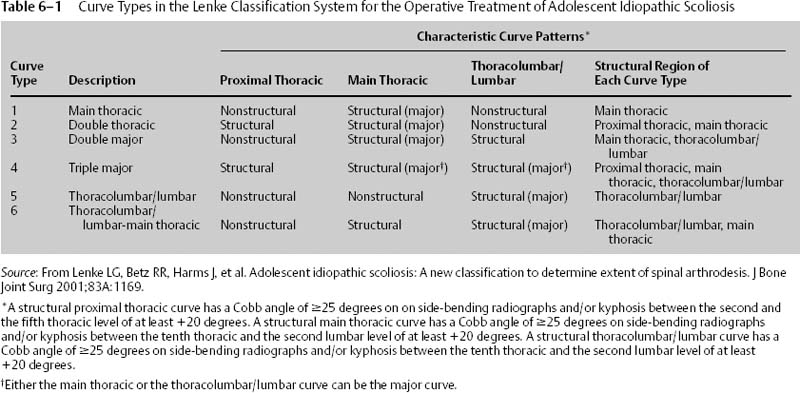
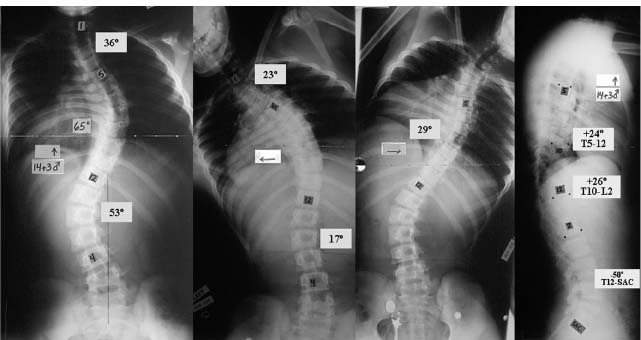
Chapter 6 The normal spine is straight in the coronal plane. In the sagittal plane, the thoracic spine averages ~30 degrees of kyphosis (range 10 to 50 degrees, measured from T5 to T12), and the lumbar spine contours to ~55 degrees of lordosis (range 35 to 80 degrees, measured from T12 to S1).1,2 Scoliosis, classically regarded as a frontal plane curvature, is a three-dimensional deformity, in which the spine deviates from the midline in the coronal plane, and the affected vertebrae rotate maximally at the apex of the curve.3 The etiologic classification of scoliosis is broadly categorized as idiopathic, neuromuscular, syndrome related, and congenital. Idiopathic scoliosis, which constitutes ~80% of patients with scoliosis, is defined as a lateral curvature of the spine for which no etiology can be established.4 Idiopathic scoliosis can be further divided according to the age upon diagnosis. These divisions, as recommended by the Scoliosis Research Society (SRS), include infantile (ages 0 to 2 + 11), juvenile (age 3 to 9 + 11), adolescent (10 to 17 + 11) and adult (≥18 years).4 Several classification schemes exist for describing the patterns of idiopathic scoliotic curves. These schemes evaluate the location and magnitude of each curve to assess different curve patterns thereby facilitating communication among treating physicians, enabling treatment recommendations, and allowing comparison of different treatment methods. The magnitude of the coronal deviation of a scoliotic curve is measured by the Cobb method as recommended by the Terminology Committee of the SRS (Fig. 6–1A).5 The end vertebrae of the curve are located on standing, long cassette posteroanterior spine radiographs. These vertebrae define the proximal and distal extent of a curve.6 They are identified as the cranial and caudal vertebrae within the selected curve that are most tilted from the horizontal. The degree of tilt between these two vertebrae defines the Cobb angle. This angle is measured by outlining the superior end plate of the cranial end vertebra and the inferior end plate of the caudal end vertebra. Perpendicular lines are then constructed at right angles to the end plates of the outlined end vertebrae. The angle formed by the intersection of the perpendicular lines defines the Cobb angle of the selected curve. If more than one curve exists, a Cobb angle measurement is made for each curve. The apex of a curve defines its center.7 It is the most laterally deviated and most horizontal vertebra or disk of the curve. A single vertebra can often be defined as the apex. If, however, a pair of vertebrae is at the apex, an apical disk is used to define the level of the apex (Fig. 6–1B). Sagittal alignment is measured by the Cobb angle between the perpendiculars to the superior end plate of the proximal vertebra and inferior end plate of the distal vertebra on standing, long cassette lateral spine radiographs. Thoracic kyphosis begins at T1; however, this vertebra is difficult to identify on lateral radiographs, therefore T5 is used as the proximal thoracic vertebra, and T12 is used as the distal vertebra. Lumbar lordosis is measured in the same manner, extending from T12 to S1 (Fig. 6–1C).8 In 1983, King et al. presented a classification system for thoracic adolescent idiopathic scoliosis (AIS).9 The benefit of this classification scheme included a treatment algorithm based on curve types that allowed surgeons to determine the appropriate curves and vertebral levels for arthrodesis. Five types of curves were described in detail. Figure 6–1 (A) Cobb measurement of scoliotic coronal plane deviation. Intersecting lines are constructed perpendicular to the superior end plate of the superior end vertebra and the inferior end plate of the inferior end vertebra. The angle subtended by the perpendiculars is the Cobb angle for the selected curve. (B) Curve apex. The apex of a curve defines its center. It is the most laterally deviated and most horizontal vertebra or disk of the curve. (C) Sagittal alignment. Thoracic sagittal alignment measured by the Cobb angle between the perpendiculars to the superior end plate of T5 and the inferior endplate of T12. (By permission from O’Brien MF, Kuklo TR, Blanke KM, Lenke LG. Spinal Deformity Study Group Radiographic Measurement Manual. Memphis, TN: Medtronic Sofamor Danek; 2004.) The King system remained the principal classification scheme for thoracic AIS for more than 20 years, guiding evaluation and treatment. However, several limitations of the King system have recently been highlighted. The system is not comprehensive, as only thoracic curves are classified. Consequently, thoracolumbar, lumbar, double, and triple major curves are not included. Additionally, all patients in King’s series received Harrington rod instrumentation that solely corrected deformity in the coronal plane. Therefore, the curves were evaluated only in the coronal plane, failing to recognize scoliosis as a three-dimensional deformity and the need to assess sagittal alignment. This approach has guided the operative assessment of scoliosis despite the advent of segmental spinal instrumentation systems that allow surgeons to treat scoliosis as a three-dimensional deformity, facilitating correction in the coronal, sagittal, and axial planes.10–14 Furthermore, the King system has demonstrated fair-to-poor interobserver and intraobserver validity, reliability, and reproducibility by two independent groups of surgeons in two separate studies.15,16 In response to these shortcomings, Lenke et al. developed a new classification system for the operative treatment of AIS.17 This new classification scheme was designed to be 1. Comprehensive and include all types of curves. 2. Two-dimensional, with increased emphasis on sagittal plane alignment. 3. Treatment-based, recommending arthrodesis of necessary curves only, allowing selective fusion when appropriate. 4. Objective, using specified criteria to differentiate individual curve types. 5. Demonstrate good-to-excellent interobserver and intraobserver reliability. 6. Easily understood and clinically practical. There are three components to the Lenke classification system: curve type, lumbar spine modifier, and sagittal thoracic modifier. Each component is assessed separately and then combined to create a classification triad (Fig. 6–2). The classification scheme uses four long cassette radiographs: standing posteroanterior and lateral, along with supine left and right side bending. Classification begins by dividing the spinal column into three regions: Figure 6–2 The Lenke Classification System for the operative treatment of adolescent idiopathic scoliosis. (From Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg 2001;83A:1169. Reprinted by permission.) 1. Proximal Thoracic (PT): apex at T3, T4, or T5. 2. Main Thoracic (MT): apex between T6 and the T11-T12 disk. 3. Thoracolumbar/Lumbar (TL/L): apex between T12 and L1 for thoracolumbar curves, and between the L1-L2 disk and L4 for lumbar curves. A Cobb measurement of the curve in each region is obtained. Curves are categorized as major or minor. The largest curve is designated the major curve. The smaller minor curves are then established as structural or nonstructural by evaluating curve flexibility and sagittal alignment. Structural curves demonstrate coronal plane rigidity 25 degrees on side-bending radiographs and/or kyphosis 20 degrees on sagittal radiographs. Regional kyphosis is measured as follows; PT (T2-T5), MT (T10-L2), TL/L (T10-L2). Six curve types can be assigned according to the identified major and minor structural curves. The defined curve types include (Table 6–1; Figs. 6–3 and 6–4): 1. Type 1, Main Thoracic (MT) 2. Type 2, Double Thoracic (DT) 3. Type 3, Double Major (DM) 4. Type 4, Triple Major (TM) 5. Type 5, Thoracolumbar/Lumbar (TL/L) 6. Type 6, Thoracolumbar/Lumbar–Main Thoracic (TL/L-MT) The MT curve is the major curve in Types 1 to 3. The TL/L curve is the major curve in Types 5 and 6. Either the MT or the TL/L curve can be the major curve for Type 4 curves. On the basis of this classification, spinal arthrodesis should include only the major curve and the structural minor curves. A lumbar spine modifier is added to assess the degree of lumbar coronal plane deformity. The center sacral line (CSL) is drawn vertically from the midpoint of S1 through the lumbar apical vertebra. When the apex is a disk, the lumbar modifier is determined by the position of the CSL in relation to the vertebra immediately above and below the apical disk. If the CSL passes between the pedicles of the apical lumbar vertebra, a lumbar modifier A is assigned. If the CSL falls between the medial edge of the concave pedicle and the lateral vertebral body, lumbar modifier B is assigned. If the CSL does not touch the lateral edge of the apical lumbar vertebra, lumbar modifier C is assigned. If a distinction between modifiers A and B or between B and C cannot be determined, modifier B should be assigned (Fig. 6–5). Figure 6–3 Lenke classification system for adolescent idiopathic scoliosis curve Types 1 to 6. The main thoracic curve is the major structural curve unless otherwise specified. Type 1 (MT, main thoracic structural); Type 2 (DT, main thoracic and proximal thoracic structural); Type 3 (DM, main thoracic and thoracolumbar/lumbar structural); Type 4 (TM, proximal thoracic, main thoracic, and thoracolumbar/lumbar structural); Type 5(TL/L, only thoracolumbar/lumbar structural); and Type 6 (TL/L-MT, thoracolumbar/lumbar major structural, main thoracic minor structural). Figure 6–4
The Lenke Classification System of Adolescent Idiopathic Scoliosis
♦ Radiographic Measurements
♦ Classification Schemes for Adolescent Idiopathic Scoliosis
♦ Lenke AIS Classification System
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


