Fig. 54.1
Prostaglandin-associated periorbitopathy. The patient has a history of the left eye only Lumigan use for a number of years and had left enophthalmos along with superior sulcus deformity due to the loss of orbital fat. Axial T2-weighted (a) and sagittal T1-weighted (b) MR images show left-sided enophthalmos with a deep superior sulcus (arrow) due to diffusely diminished orbital and periorbital fat. The patient’s unaffected right eye is shown on the sagittal T1-weighted image for comparison (c)
54.4 Differential Diagnosis
The differential diagnosis for an adult patient who presents with enophthalmos includes orbital blow-out fracture, silent sinus syndrome, scirrhous breast carcinoma metastases, localized scleroderma, and postirradiation atrophy. For example, orbital blow-out fractures can lead to enophthalmos when there is persistent orbital fat herniation through orbital wall defects or persistently displaced fracture fragments that lead to orbital cavity expansion (Fig. 54.2). While a history of trauma may be given, patients may not always recall this. Silent sinus syndrome consists of enophthalmos secondary to orbital vault expansion associated with atelectasis of the ipsilateral maxillary sinus. It can also develop after orbital trauma that damages the ostiomeatal complex. The maxillary sinus is often completely opacified, and the infundibulum is collapsed (Fig. 54.3). Scirrhous breast carcinoma metastases to the orbit can lead to retraction of the globes rather than proptosis due to desmoplastic fibrosis. These metastases can appear as infiltrative enhancing lesions (Fig. 54.4).
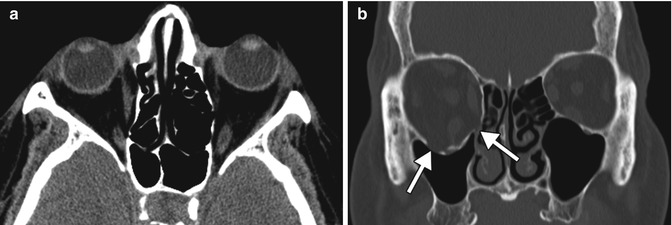
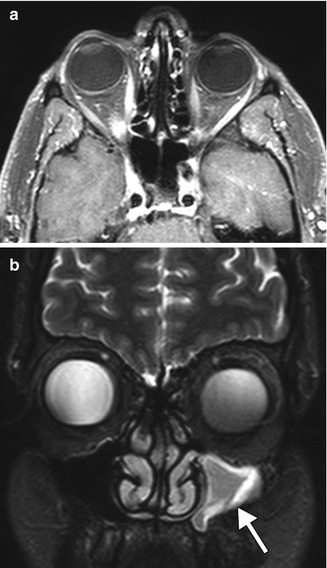
Fig. 54.2
Orbital blow-out fracture. Axial CT image (a) shows mild right enophthalmos and medial bowing of the right lamina papyracea. The coronal CT image (b) shows outward displacement of the inferior and medial orbital walls (arrows) and a relatively voluminous right orbital cavity
Fig. 54.3




Silent sinus syndrome. Axial post-contrast fat-suppressed T1-weighted MRI (a) shows left enophthalmos. The coronal fat-suppressed T2-weighted MRI (b) shows that the left maxillary sinus is relatively small in size and filled with secretions (arrow)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
