Chapter 165 Total Facet Arthroplasty
All of these studies were approved by the U.S. Food and Drug Administration (FDA) as Investigational Device Exemptions (IDE) studies; however, three of the four studies are still in the preliminary recruiting phase, with minimal published outcome data. The midterm results of the Total Facet Arthroplasty System (TFAS, Archus Orthopedics, Redmond, WA) U.S. IDE trial were published more recently and were promising.1 Although the U.S. IDE trial for the Total Posterior-Element System (TOPS, Impliant, Ramat Poleg, Israel) has commenced only more recently, the potential efficacy and safety in the management of degenerative lumbar stenosis were recently underscored in a publication analyzing early clinical outcomes in 29 patients implanted with the device outside of the United States.2
Background
When surgical intervention was first advanced as a viable treatment option for lumbar degenerative disc disease by Dandy in 1929,3 relatively little was understood with regard to spinal biomechanics. Since that time, as understanding of the underlying biomechanics of the spine has evolved, so too has the application of these principles to the surgical management of various disorders of the spine. Nowhere is this application more apparent than in nonpenetrating, blunt force trauma to the spine, in which management of the resultant stereotyped injury patterns produced in response to externally applied forces has become more intuitive through the application of biomechanical principles derived from anatomic (cadaver) and computer-assisted models. The relevance of biomechanics is not limited to trauma because the application of these same principles can also contribute to restoration of anatomic balance after iatrogenic destabilization of the spine.
The early history of lumbar surgery often involved midline, transdural approaches to the disc space. As surgical technique evolved to extradural discectomy and decompression, the surrounding ligamentous and articular structures began to represent greater barriers to adequate operative visualization. The introduction of the surgical microscope to lumbar discectomy by Yaşargil4 and Caspar5 in 1977 served to lateralize and decrease the size of the working surgical field, magnifying further the intimate anatomic relationship between the disc space, lateral recess, and facet complex. As a compensatory maneuver, partial facetectomy was eventually incorporated into the surgical technique to improve both visualization and access to the compressed neural elements. The degree of facetectomy required to achieve decompression safely varies, depending on both surgeon experience and facet joint size and orientation. In a prospective, nonrandomized study, Çelik et al.6 showed that a facet angle of less than 35 degrees does not allow for a safe surgical corridor, resulting in the need for a more extensive facetectomy.
Over the past 20 years, the use of posterior instrumented fusion, primarily with pedicle screw fixation, has increased dramatically after iatrogenic destabilization of the facet joint in the context of surgical decompression for degenerative lumbar stenosis. In some cases, the facet complex represents the primary pathology, rather than a structural impediment to adequate decompression. This is typically seen in cases of severe facet arthropathy, resulting in significant lateral recess stenosis and nerve root impingement. The more recent, controversial concept of the degenerative facet joint as an independent pain generator has also contributed to the growing trend of combined aggressive facetectomy with posterior instrumented fusion as a common surgical practice.
Whatever the underlying pathology, it is generally accepted that rigid spinal fusion permanently alters both local and global spinal biomechanics. The resultant increased, compensatory range of motion (ROM) at neighboring spinal segments after instrumented fusion leads to accelerated rates of adjacent-level degeneration—25% to 40% over 5 years—often necessitating reoperation for decompression and extension of the fusion construct.7,8 In this context, the emergence of motion preservation strategies and dynamic stabilization has garnered increasing interest in the both the neurosurgical and orthopedic literature.
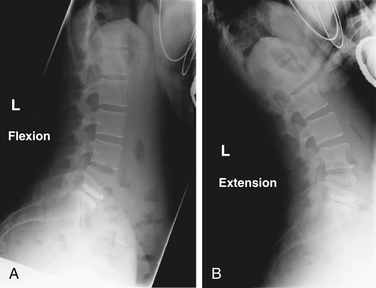
Although the concept of motion preservation is not a novel one, the potential restoration of near-normal lumbar kinematics via facet replacement systems is a relatively recent development. Approved by the FDA for single-level disc disease with associated mechanical back pain, the lumbar artificial disc (e.g., Charité, DePuy Spine, Raynham, MA; ProDisc, Synthes Spine, West Chester, PA) has steadily gained acceptance despite limited surgical indications (Fig. 165-1). In contrast to facet arthroplasty, lumbar disc replacement does not allow for direct posterior decompression of neural structures and can accelerate facet degeneration, potentially exacerbating facetogenic pain symptoms. For this reason, its use is contraindicated in patients with radiographic evidence of moderate to severe facet arthropathy.
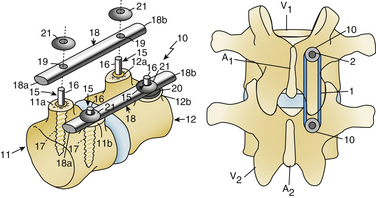
Dorsal dynamic stabilization (posterior dynamic stabilization [PDS]) devices are placed via a traditional posterior approach, allowing for direct surgical decompression before implantation. Early devices, such as the Graf ligament, were initially popular, but their popularity declined because of poor mechanical wear and issues with elastomeric material properties (Fig. 165-2). Khoueir et al.9 described a useful classification scheme for PDS devices consisting of (1) interspinous spacer devices (i.e., X STOP, Medtronic, Minneapolis, MN; DIAM, Medtronic; Coflex, Paradigm Spine, New York, NY), (2) pedicle screw and rod–based devices (i.e., Dynesys, Zimmer Spine, Minneapolis, MN; Accuflex rod, Globus Medical, Audobon, PA; Isobar, Alphatec Spine, Carlsbad, CA), and (3) total facet replacement systems (i.e., TFAS, TOPS). Although more conventional pedicle screw and rod–based PDS devices were designed to reduce facet loads and preserve intersegmental kinematics, in vitro biomechanical studies have yielded mixed results. Niosi et al.10 reported significantly increased peak facet contact forces in flexion-extension and lateral bending in cadaver human spines implanted with the Dynesys system. In theory, a facet arthroplasty system more accurately mirrors the anatomic facet joint, potentially restoring the intrinsic load-sharing properties of the intact facet complex.
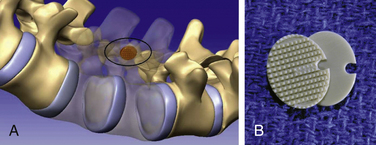
Facet joint surgeries to treat the synovial surfaces without replacing the joint itself are being investigated as well. These joint “resurfacing” technologies are in their infancy, holding the promise of treating a dysfunctional synovial joint through less invasive approaches (Fig. 165-3). Because of the lack of scientific data on these devices, they are not discussed further in this chapter.
Facet Biomechanics
Because the biomechanics of the facet joints is rarely discussed, a brief review of facet kinematics in the context of their contribution to the functional spine unit (FSU) is appropriate. The FSU refers to the three-joint structural arrangement of a single spinal level and consists of the intervertebral disc, the two facet joints and their investing capsule, and the associated posterior musculoligamentous supporting structures. The vertebrae articulate with one another via the two diarthrodial encapsulated facet joints at the superior and inferior aspects of the pars interarticularis. By virtue of their bilateral and posterior location, the facets come into maximal contact with one another during extension and axial rotation, contributing more to overall load sharing under these conditions. Generally, the orientation of the facet joint changes at differing locations throughout the spine, from a more coronal orientation with approximately 45 degrees of inclination from the horizontal in the cervical spine to a more sagittal orientation in the lumbar spine.11 These segment-specific differences in facet geometry and characteristics serve to impart differing patterns of movement at different spinal levels.
By virtue of their more sagittal orientation, the lumbar facet joints serve to provide greater resistance to axial rotation and significantly contribute to axial load bearing, in particular, with the spine in extension.11–14 The articular surface area also increases from L1 to S1, mirroring the greater shear loads in the lower spine relative to the upper lumbar spine.14 The application of eloquent computer-generated three-dimensional finite element analyses coupled with biomechanical data obtained from related in vitro human cadaver studies has furthered understanding of lumbosacral facet kinematics in response to iatrogenic destabilization. As anticipated, models replicating bilateral laminectomy and total facetectomy have shown marked increases in the angular ROM of the lumbar motion segment, under flexion-extension and axial rotation.12,15–18 However, the relative preservation of angular ROM in the context of lateral bending underscores the greater role of the anterior column in load bearing during lateral bending.19,20 Facet biomechanics also differ between individuals, by spinal level and laterality, making their biomechanics joint-specific.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


