♦ Preoperative
Operative Planning
- Review and document preoperative visual status. This will be needed for the immediate postoperative visual assessment. Formal visual field testing should be performed on all patients with visual complaints and/or optic chiasmal compression.
- Review preoperative hormonal status. Confirm normal or only modestly elevated serum prolactin (< 150 ng/mL). All patients should be evaluated by an endocrinologist prior to surgery.
- Review imaging: magnetic resonance imaging with contrast is the best modality
- Note the sphenoid anatomy and the presence and location of the intersphenoid sinus septation. This is best seen on axial imaging and provides important intraoperative correlation.
- Note the distance between the cavernous carotid arteries as seen on axial and coronal imaging. A narrow intercarotid aperture should prompt caution and a narrow initial dural opening.
- Note the relation between the normal gland and the tumor. The normal gland will enhance more brightly than the tumor and the remaining normal gland should be ipsilateral to the side of stalk deviation.
- Note the geometry of the tumor on coronal imaging. Tumors with a significant hourglass appearance may benefit from lumbar drain insertion for air insufflation during surgery.
- Note the sphenoid anatomy and the presence and location of the intersphenoid sinus septation. This is best seen on axial imaging and provides important intraoperative correlation.
Equipment
- Transsphenoidal tray
- Optional: high-speed drill, soft tissue shaver (microdebrider)
- Optional: frameless stereotaxy
- Optional: endoscopic approach in conjunction with skilled endoscopic ear-nose-throat surgeon
Operating Room Set-up
- Loupes and headlight: optional for the preparation of the nose and the initial stages of the transseptal approach
- Cautery: bipolar, Bovie, and suction monopolar
- Microscope
- The base of the microscope will be brought into the field at the top of the operative field beside the patient’s left shoulder.
- The focal length should be set between 320 and 350 mm. The assistant oculars should be set to the left of the primary surgeon.
- Endoscope: for pure endoscopic or endoscopic-assisted operations
- The 0-, 30-, and 45-degree 4-mm (outer diameter) endoscopes should be available
- A self-cleaning apparatus is essential
- Microdoppler
- Videofluoroscopy with the C-arm arranged for a lateral skull image to confirm the appropriate trajectory to the sphenoid sinus and sella turcica. Imaging also delineates the superior and inferior limits of the sella turcica. Videofluoroscopy may also be used for an encephalogram to confirm the resection of the suprasellar tumor after instillation of air via a lumbar drain.
- Frameless stereotactic image guidance. This modality is most appropriate for repeat transsphenoidal surgery.
- Microscope
Anesthetic Issues
- Blood pressure monitoring; can consider arterial line if significant bleeding is anticipated
- Orogastric tube should be inserted for gastric suctioning at the end of the operation
- Intravenous (IV) antibiotics should be administered 30 minutes prior to incision. These should be continued postoperatively if nasal packing is placed and can be discontinued when the nasal packing is removed.
- Hydrocortisone 100 mg IV preoperatively, except for patients with Cushing disease; do not give dexamethasone for antiemesis
- The endotracheal tube, temperature probe, and orogastric tubes are brought out from the left side of the mouth. No tape should be placed across the upper lip.
- Oxymetazoline is applied intranasally immediately after intubation
Spinal Drainage
- Not routinely performed; should be considered in patients with significant suprasellar component especially if there is constriction of the tumor at the level of the diaphragma sellae (hourglass tumor configuration). Place after intubation and connect to a closed drainage system. Do not drain cerebrospinal fluid (CSF) during the operation.
♦ Intraoperative (Fig. 18.1)
Positioning
- The patient is placed in a semirecumbent (lawn chair) position with the thorax elevated ~20 degrees. The patient’s right shoulder is placed at the upper right corner of the bed. With the patient’s head in a horseshoe headrest, the head is flexed laterally toward the left shoulder. The bridge of the nose should be parallel to the floor. The bed is then placed diagonally in the operating room so that the patient’s head is parallel to the walls of the room. The operating table is tilted slightly toward the surgeon.
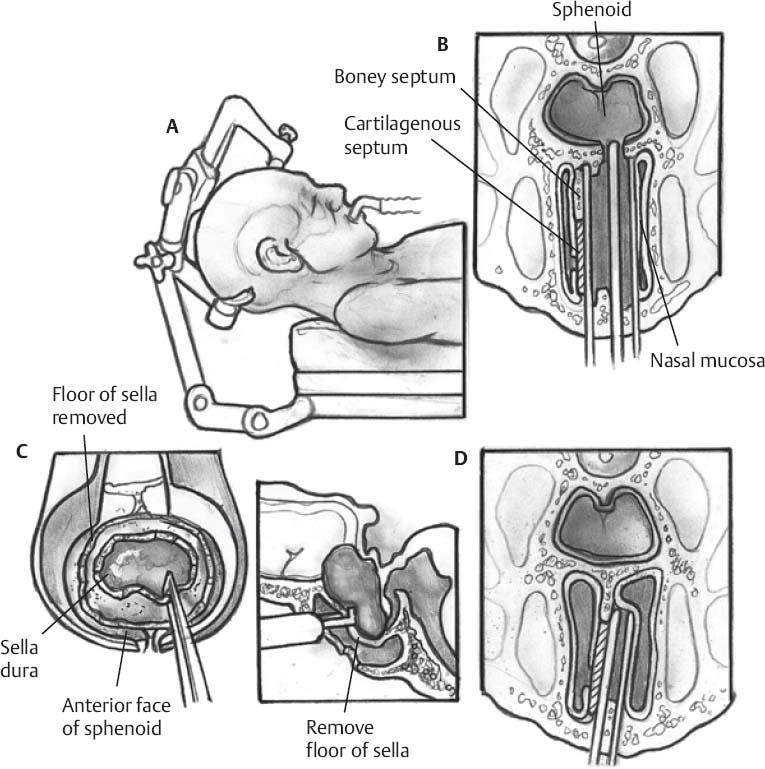
Fig. 18.1 Schematic of (A) head position and progressive transsphenoidal approach to the sella (B,C).
- Access to the periumbilical region should be provided for a possible fat graft harvest
- The operating surgeon stands to the patient’s right with the assistant to the left of the surgeon
- Access to the periumbilical region should be provided for a possible fat graft harvest
Sterile Scrub and Prep
- Betadine paint is applied to periumbilical region
- Chlorhexidine is applied to face, nose, and mouth
Approaches to the Sphenoid Sinus
Endonasal Transseptal Approach
- Indications: Adult patients undergoing first time transsphenoidal surgery who have good quality nasal tissue (especially acromegalics) in whom a wide exposure is desired.
- Although a microscope may be employed, this approach is best performed with loupe magnification and a headlight.
- Place 0.5- × 3-inch patties soaked in 0.05% oxymetazoline along the nasal septum bilaterally. Cleanse the nose and mouth with chlorhexidine. Inject the septal mucosa subperichondrially with 0.5% lidocaine with epinephrine 1:200,000 and attempt to elevate a submucosal plane by hydrodissection.
- Incision: Using a 15-blade knife in the right nostril, make a J-shaped hemi-transfixion incision at the anterior aspect of the septum extending it inferiorly onto the floor of the nasal cavity.
- Place 0.5- × 3-inch patties soaked in 0.05% oxymetazoline along the nasal septum bilaterally. Cleanse the nose and mouth with chlorhexidine. Inject the septal mucosa subperichondrially with 0.5% lidocaine with epinephrine 1:200,000 and attempt to elevate a submucosal plane by hydrodissection.
Submucosal Tunnels
- Ipsilateral submucosal tunnels: Using a Cottle or Freer dissector, develop a submucosal plane first along the ipsilateral cartilaginous septum and then the ipsilateral bony septum toward the sphenoid rostrum.
- Contralateral submucosal tunnels: Identify the junction of the cartilaginous and bony septum; whereas the cartilaginous septum feels smooth, the bony septum has a granular texture. Separate the cartilaginous septum along its attachment to the bony septum and then along the maxillary ridge. Displace the cartilaginous septum into the left nasal cavity. Develop a posterior submucosal tunnel along the contralateral bony septum toward the sphenoid rostrum.
- Insert a long speculum on either side of the isolated septal bone. Using Knight scissors and a large pituitary rongeur, resect the septal bone in the path toward the sphenoid sinus. This bone is saved for sellar reconstruction at the end of the operation. Using the blades of the speculum, out-fracture both middle turbinates to provide a wider exposure.
- An instrument is inserted into the sphenoid sinus and a videofluoroscopic image is obtained to confirm the appropriate trajectory and anatomic details.
Sublabial Transseptal Approach
- Indications: Pediatric patients. Adult patients undergoing extended microscopic skull base approaches.
- Perform the initial dissection endonasally in an identical manner to the endonasal transseptal approach.
- After fashioning the submucosal tunnels endonasally, retract the upper lip and perform a sublabial incision from canine to canine. A cuff of mucosa must remain attached to the gingiva to permit closure at the end of the operation.
- Using sharp dissection, expose the piriform aperture. Avoid liberal use of Bovie cautery to prevent thermal injury to the teeth. Develop bilateral inferior submucosal tunnels along the nasal floor and detach the cartilaginous septum from the anterior nasal spine.
- Join the sublabial incision to the endonasal tunnels and place the nasal speculum exposing the rostrum of the sphenoid.
Endonasal Septal Displacement (Direct Sphenoidotomy)
- Indications: Adult patients undergoing repeat transsphenoidal surgery or first time transsphenoidal surgery in patients with poor quality nasal tissue (especially patients with Cushing disease). This approach provides a rapid exposure of the sphenoid sinus but is narrower than the transseptal approach. The trajectory is also slightly off midline and exposes more of the contralateral side of the sella.
- This approach is performed from the outset with the microscope
- Place a long nasal speculum in the right nostril along the middle turbinate with the tips approximated 1.5 cm above the choana. Obtain a videofluoroscopic image to confirm the appropriate trajectory to the sphenoid sinus.
- Vertically incise the septal mucosal just anterior to the rostrum of the sphenoid. Displace the posterior septum from the sphenoid rostrum and retract the septum with both layers of mucosa attached into the contralateral nasal cavity. Elevate the mucosa overlying the sphenoid sinus bilaterally to expose both sphenoid ostia.
Endoscopic Binasal 3- or 4-Hand Approach
- Indications: Adult patients undergoing transsphenoidal surgery
- Although this is a binasal operation, choose the nasal cavity with the most generous working room for the initial portions of the approach. Use the 4-mm (outer diameter), 18-cm length, 0-degree endoscope for the transsphenoidal approach.
- Identify the nasal anatomy: visualize the nasal floor, inferior and middle turbinates, and choana
- Lateralize the middle turbinate and identify and lateralize the superior turbinate. Find the sphenoid ostium posterior to the superior turbinate.
- Using the suction monopolar, cauterize the mucosa surrounding the sphenoid ostium and the posterior septum.
- Detach the posterior septum from the sphenoid rostrum and displace the septum into the contralateral nasal cavity. Expose the contralateral sphenoid ostium and resect the sphenoid bone between the two ostia.
- Resect the posterior septum either using a back biting rongeur or the soft tissue shaver (microdébrider). Do not resect the posterior septum more anteriorly than the anterior limit of the middle turbinate.
- Enter the contralateral nasal cavity, identify and lateralize the middle and superior turbinates. Ensure that the posterior septectomy is complete.
Sphenoidotomy and Sellar Exposure
- If performing a transseptal approach, bring the microscope into play at this time.
- Microscopic sphenoidotomy
- The sphenoidotomy begins by removing the bone between the sphenoid ostia using a pituitary rongeur
- Using a Kerrison punch, widen the sphenoidotomy in all directions until the limits of the sella are visualized. This requires removal of intersphenoid sinus septae, if present.
- Confirm adequate exposure of the superior and inferior limits of the sella using videofluoroscopy
- The sphenoidotomy begins by removing the bone between the sphenoid ostia using a pituitary rongeur
- Endoscopic sphenoidotomy
- The sphenoidotomy must be larger than that performed for the microscopic approach to account for the presence of the endoscope in the operative field. The endoscope is situated superiorly and is “driven” by a separate surgeon. A long (30 cm) endoscope helps to keep each surgeon’s hands away from each other.
- Continue the sphenoidotomy inferiorly until a suction catheter can easily pass to the clivus below the sella. Superiorly, remove the anterior wall of the sphenoid until the planum sphenoidale is well visualized.
- Identify the carotid protuberances and opticocarotid recesses whenever possible
- The sphenoidotomy must be larger than that performed for the microscopic approach to account for the presence of the endoscope in the operative field. The endoscope is situated superiorly and is “driven” by a separate surgeon. A long (30 cm) endoscope helps to keep each surgeon’s hands away from each other.
- Sellar exposure
- If the anterior wall of the sella is thin, it can often be fractured with a blunt hook. Otherwise, an osteotome or a high-speed drill can be used to traverse the anterior wall.
- The limits of the sellar exposure are defined by the cavernous sinuses laterally, the sellar floor inferiorly (the sellar floor should be removed), and the tuberculum sellae superiorly. Superiorly, exposure does not need to extend beyond the superior intercavernous sinus.
- If the anterior wall of the sella is thin, it can often be fractured with a blunt hook. Otherwise, an osteotome or a high-speed drill can be used to traverse the anterior wall.
Dural Opening
- Prior to opening the dura, re-review the preoperative imaging. Identify the location of the normal gland (if discernible) and determine the intercarotid distance at the level of the cavernous sinus. If a narrow interval is present, use the microdoppler to ensure that the carotid arteries have not been exposed.
- Open the dura with a fine knife. Care should be taken to only traverse the dura and to not enter the gland or tumor. Remove a patch of dura when resecting macroadenomas so that the specimen can be sent to pathology to determine the presence of tumor invasion. A cruciate incision is made when removing microadenomas. If the intercarotid distance is narrow, open the dura first with a midline vertical incision and then carefully complete the horizontal incision after using the microdoppler.
Removal of Tumor
- Using a blunt nerve hook, develop a subdural plane between the dura and the tumor
- Remove the tumor sequentially using angled ring curettes, pituitary forceps, and suction. Initially debulk the inferior portions of the tumor, followed by the lateral wings toward the cavernous sinuses, and finally the superior portions toward the diaphragma sellae.
- If the diaphragma does not descend into the sella, jugular compression or Valsalva maneuver may displace the suprasellar portions of the tumor into the sella. Alternatively, if a lumbar drain has been inserted, inject 10 mL of air over 10 seconds.
Closure
- Irrigate the tumor cavity with saline; carefully inspect for the presence of a CSF leak
- Closure of the sella turcica
- If no CSF leak is present, place an absorbable gelatin sponge within the tumor cavity. Reconstruct the sellar floor using either harvested septal bone or a synthetic material; these should be placed in an extradural plane if possible.
- If a CSF leak is present, harvest periumbilical fat. Soak the tailored pieces of fat in antibiotic solution and then dab them in cotton and Avitene. Place the fat grafts into the tumor bed and reconstruct the sellar floor. Large defects in the diaphragma sellae also require obliteration of the sphenoid sinus with fat.
- To prevent overpacking of the sella, confirm that the brain pulsations continue to be transmitted through the packing material.
- If no CSF leak is present, place an absorbable gelatin sponge within the tumor cavity. Reconstruct the sellar floor using either harvested septal bone or a synthetic material; these should be placed in an extradural plane if possible.
- Closure of the nasal phase
- Transseptal approaches. Remove the speculum, medialize the outfractured middle turbinates, and reposition the septum in the midline. Place nasal rockets between the middle turbinates and the nasal septum. Close the hemitransfixion incision (and the sublabial incision if present) using absorbable chromic suture.
- Direct sphenoidotomy. Remove the speculum and irrigate the nasal cavity. Medialize the ipsilateral middle turbinate and reposition the nasal septum in the midline. No nasal rockets are required.
- Endoscopic binasal approach. Irrigate the nasal cavities and inspect around the inferolateral corners of the sphenoidotomy for bleeding. Medialize the middle turbinates bilaterally. No nasal rockets are required.
- Suction the nasopharynx and oropharynx. Suction the stomach using the preoperatively placed orogastric tube.
- Transseptal approaches. Remove the speculum, medialize the outfractured middle turbinates, and reposition the septum in the midline. Place nasal rockets between the middle turbinates and the nasal septum. Close the hemitransfixion incision (and the sublabial incision if present) using absorbable chromic suture.
♦ Postoperative
- Examine visual fields as soon as possible postoperatively.
- Steroids: Patients who are adrenally insufficient preoperatively should be continued on steroids postoperatively. If not adrenally insufficient preoperatively, discontinue the hydrocortisone after the morning dose on the first postoperative day. Draw the serum cortisol level at 6 AM on postoperative day 2 and 3. Levels less than 8 mcg/dL require steroid replacement.
- Continue antibiotics until nasal packing is removed on postoperative day 1.
- Monitor for diabetes insipidus. Strict fluid input and output measurements; daily weights on the same scale; serial urine specific gravity, serum sodium, and serum and urine osmolarity. Greater than 300 mL of urine output for 3 consecutive hours should prompt an evaluation. Treat diabetes insipidus acutely with intravenous or subcutaneous desmopressin. If persistent, may use either intranasal or oral desmopressin.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue








