59 Trauma to the Brain
General Principles of Head Injury Care
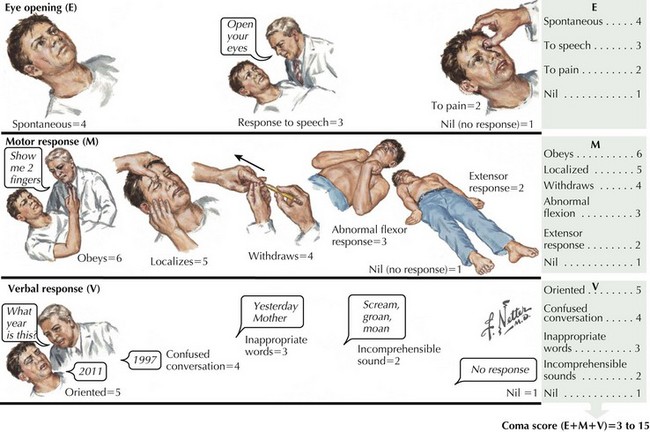
Concomitantly, the patient’s general level of responsiveness must be assessed using the Glasgow Coma Scale (Fig. 59-1). The lowest possible score of 3 means that individuals have no ability to open the eyes, no motor response to verbal command or direct stimuli, and no verbal response to the physician’s questions, giving a score of 1 or nil for each of the three components. The highest possible score is 15. Soft tissue injuries are commonly associated with more severe head injuries. A complete examination of the exterior surface of the face and head is vital. Blood loss can be extensive given the location of blood vessels within the dense connective tissue of the scalp, which decreases retraction of cut vessels and promotes bleeding.
Skull Fractures
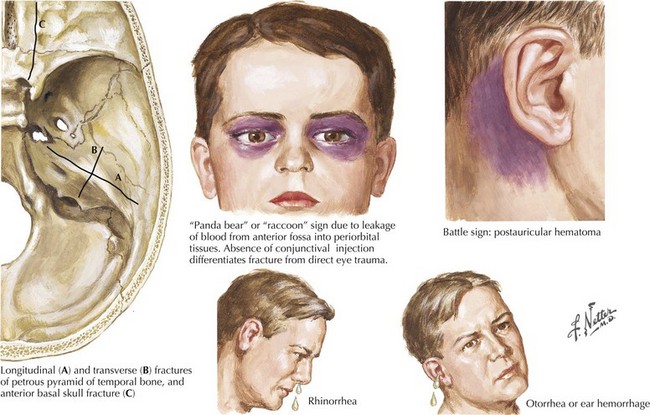
These can be located in the calvaria (vault) and/or the basal skull. Fractures of the cranial vault carry a 20 times greater incidence of intracranial hematoma in comatose patients and a 400 times greater incidence in conscious patients. Basal skull fractures, often difficult to identify on head CT, can present with pathognomonic signs, including raccoon or Panda bear eyes, battle signs (ecchymosis over the mastoid), and cerebrospinal fluid (CSF) leakage from the nose, throat, or ears (Fig. 59-2). Most leaks resolve spontaneously. Persistent leaks necessitate operative treatment (Fig. 59-3).
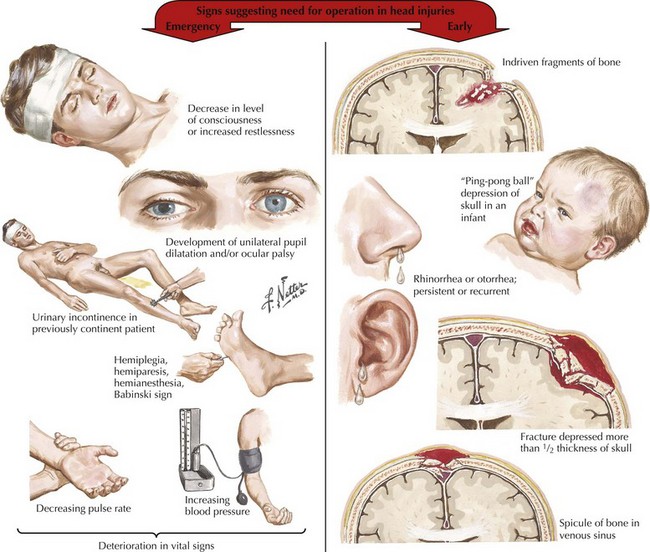
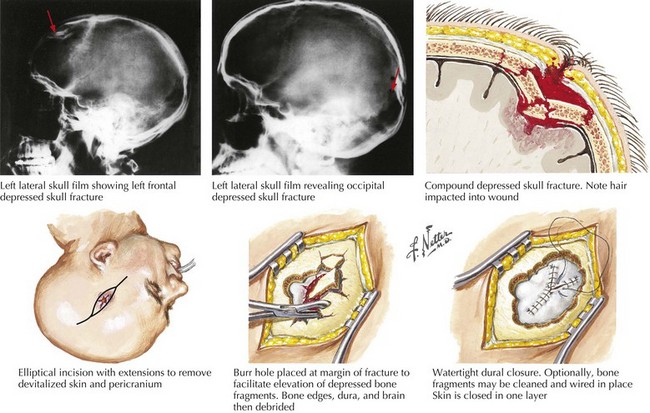
Depressed fractures, and those along the temporal bone, are more commonly associated with injury to the brain or blood vessels. A fracture line across the middle meningeal artery may predispose to an epidural hematoma. Open fractures with their communication between the intracranial vault and the external environment are associated with higher risks of spinal fluid leaks and infection (Fig. 59-4).
Extra-Axial Traumatic Brain Injuries
Epidural Hematomas
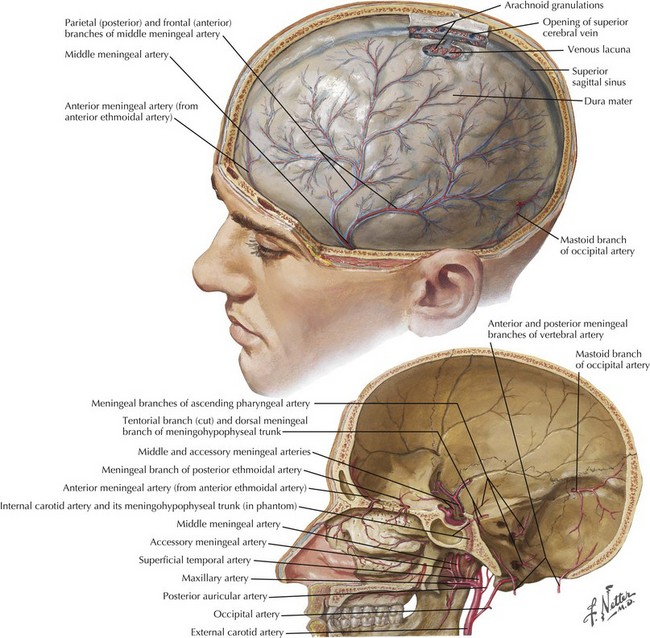
These represent an acute blood collection contained between the dura and inner table of the skull. These occur in approximately 2% of TBIs (Fig. 59-5). Epidural hematomas (EHs) most commonly develop in the temporal and parietal regions; 90% of EH are associated with a skull fracture. Arterial lacerations, particularly of the middle meningeal artery (Fig. 59-6) or, less commonly, venous injuries, initiate the formation of hematomas. Contiguous lacerations of the dura mater allow this blood into the epidural space.
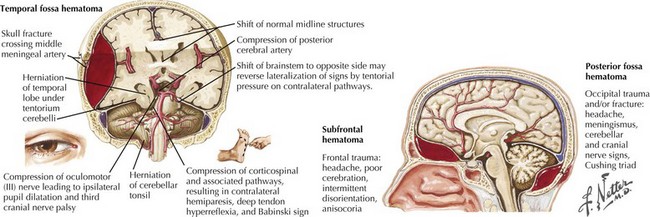
Immediately after the closed head injury, the patient “typically” experiences an initial but relatively brief loss of consciousness secondary to the primary concussive injury. This is then followed by a lucid interval with return of wakefulness. Subsequently, as the torn vessels leak, an epidural hematoma develops and enlarges, leading to a rapid lapse into coma. Sometimes this entire process may transpire from injury, to transient loss of consciousness, and to a brief period of a “paradoxically reassuring alertness,” only to have a devastating, often irreversible, coma develop within just 1 hour after the blunt head injury (see Fig. 59-3). However, this classic presentation occurs in less than one third of affected individuals. The actual rate of symptom progression depends on the type of associated brain injuries, their etiology, and the subsequent precise rate of blood accumulation within the epidural space.
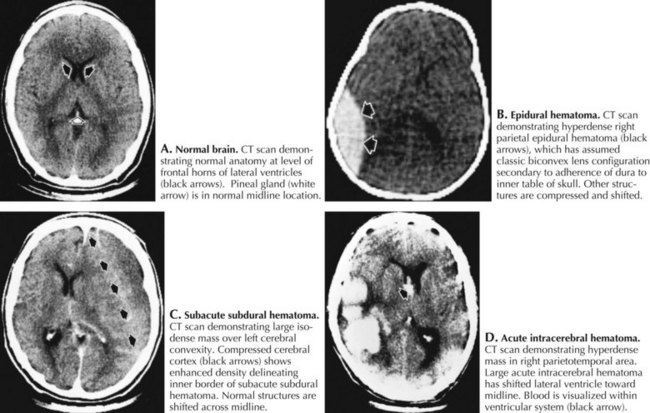
Cranial CT imaging usually demonstrates a hyperdense, biconvex collection between the skull and brain (Fig. 59-7). On occasion, the initial CT is normal as the hematoma has yet to develop to a size that is definable. Thus when the patient is “at risk,” it is essential to be prepared to repeat the CT scan at the slightest change in clinical status. Once the EH is identified, emergency surgical evacuation is indicated. Any failure to recognize an epidural hematoma has a most significant mortality depending on patient age, time of treatment, hematoma size, and associated injuries.
Acute Subdural Hematoma
These blood collections are located between the brain parenchyma and the dural membranes and are classified by their temporal profile. Acute subdural hematomas (SDHs) occur in 15% of TBI patients; these are seven to eight times more common than epidural hematomas. Older individuals are at greater risk because as the brain ages, there is an innate atrophy of the cerebral cortex. Thus in seniors, as the brain “normally” lessens in volume, an increasing space develops within their subdural compartment. In turn this leads to increased stretch on the bridging veins between the skull and the cerebral surface (Fig. 59-8






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


