CHAPTER 336 Traumatic and Penetrating Head Injuries
In recent years there has been an apparent paradigm shift of scientific interest in the long-term effects of mild traumatic brain injury (MTBI) and its contribution to posttraumatic stress disorder (PTSD).1–6 It is estimated that more than 320,000 American soldiers may have sustained TBI in Operation Iraqi Freedom (OIF),4 the majority of which were mild, contributed to PTSD and physical ailments, and thus had the potential to disrupt postwar American lives.1,3,5,7–9 We have also witnessed major initiatives by the U.S. government to support the neuroscience community in its attempts to better understand the pathogenetic mechanisms, manifestations, and more effective management of TBI and PTSD caused not only by PBI but also by blast overpressure generated by complex explosive devices.4,10–14 Newly designed protective body armor has reduced the incidence of PBI significantly.4,15 However, the nature of the asymmetric warfare during OIF has exposed military personnel to sophisticated explosive devices generating blast overpressure that results in secondary cellular and molecular insults to the brain parenchyma akin to diffuse brain injury.4,11–13,16,17 Significant progress has been made in achieving a more detailed understanding of the manifestations of vascular insults and diffuse brain edema, some of which can be managed effectively by endovascular interventions and decompressive craniectomy.11,17–20
The biomechanics of civilian gunshot wounds to the head (GSWHs)21–36 tends to be different from that of military craniocerebral battle wounds and blast overpressure.4,5,10–13,16,17,21 Translation of kinetic forces into injury to the brain parenchyma in civilian GSWHs is direct and devastating with no hope of rescue in the majority of victims.21,22,37 When compared with military conflicts,38 civilian GSWHs have unacceptably high mortality.39 Only 18% of GSWH victims in Hernesniemi’s service were cared for by a neurosurgeon,25 and only 28 of 143 subjects in Kaufman and colleagues’ study underwent craniotomy.40 More than 90% of civilians sustaining GSWHs die—almost two thirds of them at the scene.39 In 2000, 250 people sustained GSWHs in the state of Maryland (unpublished data), 222 (89%) of whom eventually died (177 at the scene and 45 in the emergency departments of eight trauma centers). Only 10 patients were seen at the trauma resuscitation unit of the Shock Trauma Center alive; 8 of the 10 underwent surgery, and 6 (2.4%) eventually made a favorable recovery. This grim prospect has also been the general impression of other investigators.21,41–43
Ballistics, Wounding Energy, and Pathogenesis
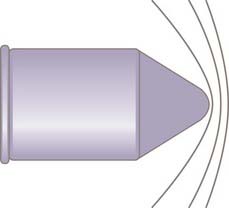
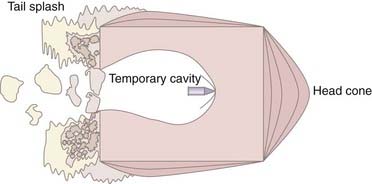
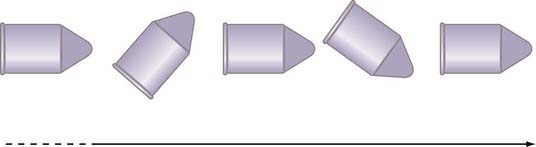
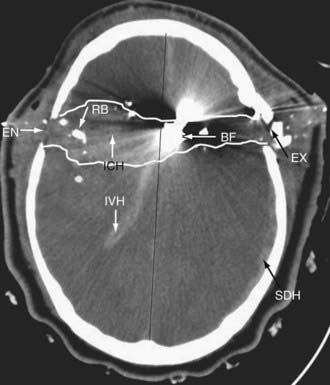
There are three components to ballistics: (1) interior, (2) exterior, and (3) terminal. Interior ballistics is defined as the science of motion of a projectile through a gun barrel as a result of combustion and expansion of a powder charge, a science extensively studied in the early 18th century by the British scientist Benjamin Robins and the Anglo-American researcher Benjamin Thompson.44,45 Exterior ballistics is the projectile’s behavior in a medium such as air and is dependent on the projectile’s shape, caliber, weight, initial velocity, and ballistic coefficient. Niccolo Tartaglia and Galileo defined the parabolic trajectory of a bullet in space until it loses all of its kinetic energy.44–50 The behavior of a projectile on impacting its target is termed terminal ballistics. Factors important in terminal ballistics include penetration, tissue density, fragmentation, detonation, shape of the charge, blast overpressure, combustion, and incendiary effect.44–46,48,50 The science of ballistics has evolved considerably since 1411 when the first matchlocks appeared in Europe. The introduction of rifling in 1520, elongated bullets by Delvigne in 1841, minié bullets in 1847, and breech loading and coated bullets in the 1850s resulted in projectiles with velocities greater than 2000 ft/sec (615 m/sec).44,45,50–52 The wounding energy (E) of a projectile depends mainly on its weight and velocity; hence, E =  M(VI2 − VR2), where M is the projectile’s weight, VI is the impact velocity, and VR is the residual velocity if the projectile has a perforating mode.45,53 The small-firearm injuries encountered in civilian GSWHs follow conventional ballistic rules of wounding energy; however, when the velocity of a projectile crosses 700 m/sec, the wounding energy depends on the power (P) of the projectile and is expressed as P = MV3. Many of the victims in the vicinity of a cased explosive or an improvised explosive device (IED) will incur injuries by fragments with a velocity of greater than 700 m/sec and low ballistic coefficient. Translation of kinetic energy into tissue damage is brought about by the tremendous amount of crushing pressure exerted on the brain parenchyma. Juxtamissile pressure affects the brain tissue immediately in the path of a projectile and may be in the thousands of atmospheres. Longitudinal strong shock waves (Fig. 336-1) start immediately after impact of the projectile with brain tissue and travel in spheres ahead of the projectile with velocities in excess of 1460 m/sec.54 Shock waves last up to 10 µsec and measure up to 80 atm. Ordinary pressure waves measuring up to 20 to 30 atm are generated as the projectile transfers its kinetic energy to the surrounding brain tissue and produces a temporary cavity.54 The negative pressure generated by the temporary cavity can suck contaminated material into the cavity, which must be débrided during surgical management of the permanent cavity.45,54,55 Experiments with 20% gelatin have indicated that as the projectile is dissecting its way through a gelatin cube, it produces a head cone and a tail splash (Fig. 336-2).55,56 Tissue density is critical in defining parenchymal damage. Solid organs such as the brain have tissue densities up to 800 times that of air, thus giving high-velocity bullets explosive power.52 The sectional area defines the impact surface of a projectile and is determined by the shape and flight characteristics of a projectile, including yaw (Fig. 336-3), spin, precession, tumbling, nutation, and drag, all of which determine the ballistic coefficient.44–51,54,56–58 GSWHs, being contact or near-contact injuries, not only plow through the brain but also deposit a tremendous amount of energy that disrupts brain tissue and major blood vessels, displaces the brainstem, arrests cardiorespiratory function, and results in instantaneous death in more than 70% of victims (Fig. 336-4).31–3354
M(VI2 − VR2), where M is the projectile’s weight, VI is the impact velocity, and VR is the residual velocity if the projectile has a perforating mode.45,53 The small-firearm injuries encountered in civilian GSWHs follow conventional ballistic rules of wounding energy; however, when the velocity of a projectile crosses 700 m/sec, the wounding energy depends on the power (P) of the projectile and is expressed as P = MV3. Many of the victims in the vicinity of a cased explosive or an improvised explosive device (IED) will incur injuries by fragments with a velocity of greater than 700 m/sec and low ballistic coefficient. Translation of kinetic energy into tissue damage is brought about by the tremendous amount of crushing pressure exerted on the brain parenchyma. Juxtamissile pressure affects the brain tissue immediately in the path of a projectile and may be in the thousands of atmospheres. Longitudinal strong shock waves (Fig. 336-1) start immediately after impact of the projectile with brain tissue and travel in spheres ahead of the projectile with velocities in excess of 1460 m/sec.54 Shock waves last up to 10 µsec and measure up to 80 atm. Ordinary pressure waves measuring up to 20 to 30 atm are generated as the projectile transfers its kinetic energy to the surrounding brain tissue and produces a temporary cavity.54 The negative pressure generated by the temporary cavity can suck contaminated material into the cavity, which must be débrided during surgical management of the permanent cavity.45,54,55 Experiments with 20% gelatin have indicated that as the projectile is dissecting its way through a gelatin cube, it produces a head cone and a tail splash (Fig. 336-2).55,56 Tissue density is critical in defining parenchymal damage. Solid organs such as the brain have tissue densities up to 800 times that of air, thus giving high-velocity bullets explosive power.52 The sectional area defines the impact surface of a projectile and is determined by the shape and flight characteristics of a projectile, including yaw (Fig. 336-3), spin, precession, tumbling, nutation, and drag, all of which determine the ballistic coefficient.44–51,54,56–58 GSWHs, being contact or near-contact injuries, not only plow through the brain but also deposit a tremendous amount of energy that disrupts brain tissue and major blood vessels, displaces the brainstem, arrests cardiorespiratory function, and results in instantaneous death in more than 70% of victims (Fig. 336-4).31–3354
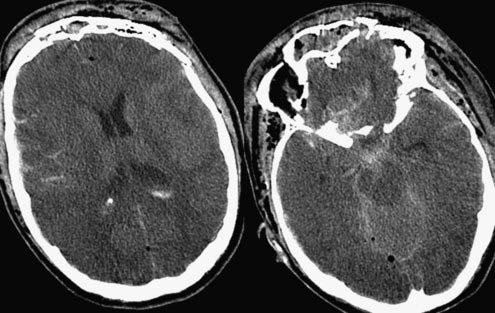
The science of ballistics and quantification of the wounding energy in cased ammunitions and complex explosives, such as car bombs and IEDs, is much more unpredictable in that it is a combination of primary blast overpressure, PBI, and closed head injury.4,10,11,13,16 Although injuries during the American Civil War were primarily due to bullets, injuries in subsequent international and regional conflicts have been caused to a major extent by shell fragments.55,59–64 In a recent presentation at the annual meeting of the conference on Advanced Technology Applications for Combat Casualty Care (ATACCC) in Florida, Bell and coauthors reported that 228 of 408 patients who sustained TBI in OIF suffered PBI and 139 had closed head injury.65 In 229 patients the predominant mechanism was exposure to complex explosive devices, which resulted in significant blast overpressure on the brain parenchyma in addition to PBI and closed TBI (Fig. 336-5). Additional mechanisms behind TBI in modern warfare and terror attacks include thermal and ischemic injuries and energy sources not appreciated in a typical measurement spectrum, such as electromagnetic energy.4,10,11 Fragments tend to most commonly be low-velocity spall (see Fig. 336-7).4,10,11,60,63,66–70 This spall can emanate from the casing of the explosive device and from packed supplemental bolts, nails, ball bearings, or the metal from a vehicle-borne explosive (i.e., a car bomb). In some cases this spall can also contain body parts of the suicide bomber, window frames, glass, gravel, or in-driven bone fragments acting as secondary impacting fragments. When such explosives impact a patient, the results vary. Factors such as proximity to the explosion, protection by both personal and vehicular armor, and the effect of the environment are all important.4 Open field explosions are less likely to have the effect of reverberating pressure waves, building collapse, or fragmenting glass, as is commonly seen when victims are located within a closed structure.4 Explosions occurring within a closed space are particularly lethal because of the proximity to the explosion, the incendiary nature of the blast, and the reverberation of the blast force.4,10,16 This lethality is commonly witnessed in bombs detonated in buses, trains, planes, and enclosed buildings.69,70 The number of survivors is typically inversely proportional to the size of the enclosure, with bus bombs having the highest lethality.69
Pathology
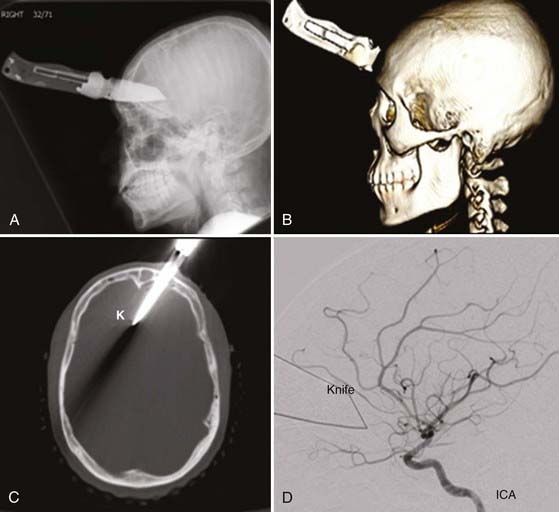
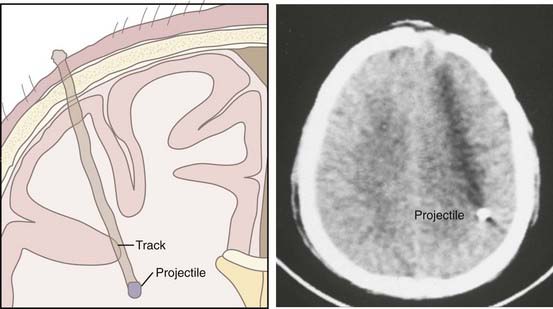
Low-velocity sharp objects, which lack any definable ballistics, penetrate the scalp, skull, and dura and lacerate the brain parenchyma, including the cortex, subcortical white matter, basal ganglia, and diencephalon or brainstem and any blood vessels in their path (Fig. 336-6).71,72 Similarly, low-velocity projectiles from artillery shells, IEDs, and spent bullets cut into the brain just like sharp objects do (Fig. 336-7). The focal motor, cognitive, and behavioral consequences of these injuries depend on the neuronal circuitry that is interrupted and the completeness of injury to blood vessels, hence producing subarachnoid hemorrhage, intracranial hematomas or traumatic intracranial aneurysms (TICAs), and arteriovenous fistulas (AVFs).71–83
The pathology with contact or near-contact injuries by civilian GSWHs is much more devastating.23,27,40,41,84 In a detailed necropsy study of 254 patients who died of firearm injuries, Freytag noticed single-track injury (permanent cavity) from ricochets in 82% of cases and multiple tracks in the remaining cases. In her study an ischemic ring was seen surrounding the permanent cavity and was topped by a layer of small hemorrhages from disruption of blood vessels.23 A robust class III literature indicates that in victims of civilian GSWHs who survived the initial injury to reach a trauma center, the path of penetration and the extent of brain injury defined the mortality. The mortality was 48% after lobar injuries,22,31,41,42,85,86 72% after unilateral multilobar injuries,22,31,35,43 77% if the midsagittal plane was crossed,22,30,31,40–43,87 84% if the midcoronal plane was crossed,86,87 and 96% if both the midsagittal and midcoronal planes were crossed.86,87 In 2000, 45 patients survived long enough to reach one of the eight trauma centers in the state of Maryland. Of the 24 patients admitted to the shock trauma center, 10 survived: 2 of 12 patients with perforating, 5 of 9 patients with penetrating, and 3 of 3 patients with tangential injuries. The relationship of the injury mode to mortality was also reflected in 816 soldiers from the Iran-Iraq War.88 In this study the proportion of patients who survived a median of 41 hours to reach an academic center were as follows: 54.8% with penetrating, 22.4% with tangential, and 7.5% with perforating injuries. The incidence of intracranial hematomas differs between reports: acute subdural hematoma, 3% to 56%27,42; intracerebral hematomas, 4% to 37%24,42; intraventricular hematoma, 1% to 56%24,27; and subarachnoid hemorrhage, 9% to 78%.21,35
In soldiers with varying amounts of body armor, the pattern is quite different. What had previously been fatal PBIs now become treatable brain injuries as a consequence of secondary damping of energy by the helmet.4,11,15 The energy absorbed by the helmet results in mechanical deformation of the inner and outer protective covering of the shield. The outer deformity tends to be smaller and focal and rarely completely penetrates, whereas the inner deformity tends to have a broader base with less depth and also rarely penetrates. The deformation of the inner aspect of the helmet may impact on the underlying scalp, transfer energy to the skull, and deform the calvaria and intracranial compartments. A piston-like deformity of this inner table can lead to a stellate scalp laceration with a severe abrasion or burn, and the resulting impact on the skull leads first to a fracture and loss of anatomic continuity of the skull. In extreme cases, commonly seen after an IED impact, the dura is violated and the local cerebral tissue will be contused by both blunt trauma and secondary impacting fragments of bone or body armor (or both). These fragments of bone typically course in a radial direction from the point of impact. Traveling perpendicular to the cortical vasculature underlying the sulci and gyri, they disrupt the vessels in their path (Fig. 336-8).
Military personnel incurring complex injuries from explosive devices sustain blast overpressure and penetrating or closed head injuries.4,11,13,16 Reporting on 234 American soldiers who were evacuated a mean of 7.4 ± 8.6 days after their war injuries, Bell and coauthors noted severe head injury (Glasgow Coma Scale [GCS] score <9) in 61 (26%).65 It was projected that a significant proportion of wounded OIF soldiers suffered from high-frequency low-amplitude or low-frequency high-amplitude shock waves, which rendered these injuries much more complex to comprehend.4,10,16 Low-intensity blast waves are not necessarily accompanied by pulmonary or gastrointestinal injuries. Because disruptive energy is transmitted to the brain with complex and high-energy blasts and may even occur through major blood vessels, TBI is not prevented by a protective helmet.10 High- and low-frequency blast waves disrupt the blood-brain barrier and produce massive brain swelling in a very short time,89–92 thereby necessitating urgent decompressive craniectomy, and when low in energy, such blast waves may result in cytoskeletal and diffuse axonal injury that leads to neurodegeneration.4,10,11,20,93
Clinical Findings
Demographics
Most patients involved in civilian GSWHs are males (87%) in the third to fourth decade of life and are nearly equally divided between homicides (50%) and suicides (46%), with a small percentage being due to accidents (4%). Almost 78% of the victims of homicide are black; 86% of the victims of suicide are white.21–25,28–32,34,36,39,42,84,94–98 Unpublished data from the Trauma Registry of the R. Adams Cowley Shock Trauma Center indicate that from 2000 through 2005, of the 333 patients admitted with civilian GSWHs, only 34 were female.99 The mean age was 30.6 ± 14.4 years, 214 were black, 100 were white, and 19 were other races. The GSWHs occurred concomitant with injuries to the face in 165, the upper extremity in 94, the thorax in 74, the lower extremity in 51, the neck in 45, the spine in 43, and the abdomen in 42 patients. The Injury Severity Score (ISS) was 31 ± 16, the head Abbreviated Injury Score (AIS) was 4.7 ± 0.7, and the Trauma Injury Severity Score (TRISS) was 0.52 ± 0.4. Military victims of PBI tend to be younger,59,60,63,64,88,100 and in OIF the mean age was reported to be 24.7 years.65
Level of Consciousness
When sharp objects,71,72,76,79,83 low-velocity spall,59,60,63,64,66,100 and spent bullets penetrate the brain, they may cause focal deficits; however, if they do not disrupt the neuronal circuitry in the brainstem tegmentum or ascending reticular activating system, they may not cause a depressed level of consciousness or coma.18,27,71,72,76,79,83,101–108
In civilian PBI an altered level of consciousness is the rule.* In a prospective study of 100 civilian GSWHs by the Barrow Neurological Institute, Grahm and associates reported postresuscitation GCS scores to be 3 to 5 in 58 patients, 6 to 8 in 8 patients, 9 to 12 in 12 patients, and 13 to 15 in 22 patients.41 Unpublished data from the University of Maryland Trauma Registry in Baltimore showed 333 patients with GSWHs in the period 2000 to 2005.99 Of these 333 patients, 187 (56%) had a GCS score of 3 to 5, 31 (9%) a GCS score of 6 to 8, 20 (6%) a GCS score of 9 to 12, and 95 (29%) a GCS score of 13 to 15. Similarly, Liebenberg and coauthors reported a GCS score of 3 to 8 in 70.4% of their patients evaluated from West Sussex England (Fig. 336-9).28
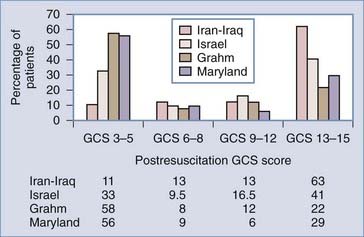
FIGURE 336-9 Stratified admission Glasgow Coma Scale (GCS) scores of victims of penetrating brain injury from the frontlines of the Iran-Iraq War, the Israeli involvement in Lebanon, and civilian gunshot wounds to the head (see references 41, 60, 66, 99).
Military experience in recent years has recorded varied levels of consciousness at the time of arrival at a medical facility. In 1990, Aarabi reported the functional outcomes of 435 patients from the Iran-Iraq War.66 In that study, 274 (63%) patients were admitted to a tertiary hospital with a GCS score of 13 to 15, 57 (13%) with a GCS score of 9 to 12, 58 (13%) with a GCS score of 6 to 8, and 46 (11%) with a GCS score of 3 to 5. In 1991, Brandvold and coworkers, reporting on 113 war casualties from the Israeli involvement in Lebanon, recorded 41% with a GCS score of 13 to 15, 16.5% with a GCS score of 9 to 12, 9.5% with a GCS score of 6 to 8, and 33% with a GCS score of 3 to 5.60 Natural selection by prolongation of time at the scene may explain some of the differences. In the Iran-Iraq War, time after injury to admission to the tertiary academic facility was 49 hours, whereas in Israel the average time at the scene was 2 hours.60,110 Bell and colleagues recorded the following GCS scores in 234 patients from OIF who were treated by neurosurgeons within 0.5 to 1.5 hours of their injury and evacuated to the continental United States (CONUS) within 7 days of their injury, with the last 38 patients arriving in CONUS within 4 days of their injury: GCS scores of 12 to 15 in 103, 9 to 11 in 70, 6 to 8 in 37, and 3 to 5 in 24 subjects.65 In a report presented by Ling, almost 20% of the military personnel deployed in OIF were subject to TBI; however, only a minority suffered secondary blast injuries and had a very low GCS score.4
Brainstem Function
Checking for brainstem dysfunction (i.e., abnormal pupillary response to light, corneal and doll’s eye reflexes, cold calorics, cough and gag reflexes) is particularly important in civilian GSWHs and military PBIs. These injuries reflect damage by either brain shift secondary to a temporary cavity resulting from ordinary pressure waves54 or uncontrollable intracranial hypertension secondary to swelling or hematomas and hence are of major prognostic significance.38,54,57,111,112 With regard to the pupils, one has to consider end-organ injury resulting from the bullet tracking around the orbital apices and cavernous sinuses. In the report of Grahm and associates, 95% of the patients with GCS scores of 3 to 5 did not exhibit any pupillary reaction, whereas in patients with higher scores, a lack of reaction was noticed in only 50%.41 In the series of Kaufman and coworkers, 30 of 38 patients with no abnormal pupillary response to light survived, but only 1 in 70 survived if both pupils were not reactive to light.40 Stone and colleagues believed the GCS score to be much more valuable in predicting outcome than the pupillary reaction to light was.35
Focal Deficits
Depending on the entrance site, a persistent focal neurological deficit is quite common in the survivors of GSWH or military PHI. In 1872, Mitchell described 7 individuals with cranial nerve injuries, including 4 with facial nerve injuries, after GSWHs during the American Civil War.113 Stookey and Scarff reported 72 instances of facial nerve injuries in 153,537 war casualties during 1917 and 1918.114 Orbital injuries during World War I (WWI) were the subject of extensive discussion by Lagrange.115 Examining injuries during World War II (WWII), Jefferson and Schorstein reported 14 patients with complex trigeminal damage,116 and Lathrop reported 150 patients with facial nerve damage.117 The incidence of visual field cuts in the Vietnam Head Injury Study (VHIS) cohort as reported by Salazar and colleagues was 13.7%.118 Eighty of 1303 casualties from the Iran-Iraq War had cranial nerve involvement: the optic nerve or globe in 60, the olfactory nerve in 24, the oculomotor nerve in 23, the abducens nerve in 13, the trochlear nerve in 11, the trigeminal nerve in 10, the facial nerve in 7, the vestibulocochlear nerve in 3, the glossopharyngeal nerve in 3, the vagus nerve in 3, and the hypoglossal nerve in 2.119 Mohr and colleagues studied speech involvement and recovery in 244 of 1030 casualties from Vietnam (VHIS cohort).120 The authors reported that sensorimotor aphasia usually changed to motor aphasia; the motor aphasia disappeared and the sensory aphasia persisted. Aphasia correlated with a bullet as the cause (versus a fragment, P < .03) and initial loss of consciousness (P < 10−6). In the same study the incidence of paresis was 28% (292 of 1030 casualties). Smutok and coauthors reported that 55% of patients in the VHIS cohort had recovered from the hemiparesis 15 years after their missile head wound.121 The incidence of motor deficits, visual field cuts, and speech difficulties in the casualties from the Iran-Iraq War was 34.6%, 13.7%, and 6.1%, respectively.3
Mild Traumatic Brain Injury, Blast, and Posttraumatic Stress Disorder
More than 320,000 OIF soldiers (20% of the deployed force) may have suffered varying degrees of TBI.130 Although the functional, cognitive, and psychological consequences of penetrating and closed head injuries incurred in armed conflicts have been extensively investigated over many years,13,38,54,59,63,66,100,118,122–129 there is no clear understanding of the exact pathogenetic mechanisms and epidemiology of MTBI and PTSD as a consequence of blast overpressure.4,11–13,16–18,65
Experimental studies indicate that blast waves have some of the characteristics of complex Friedlander waves. Blast waves rise instantaneously to a peak overpressure and decay exponentially, followed by a negative phase. Blast waves interact with the central nervous system directly through the cranium or indirectly through oscillating pressure in fluid-containing large blood vessels.10,130 Protective body armor does not prevent the interaction of brain parenchyma with shock waves.4,10 High-frequency (0.5 to 1.5 kHz) low-amplitude stress waves damage the blood-brain barrier, and low-frequency (<0.5 kHz) high-amplitude shear waves damage the gray-white matter junction. The result is brain edema, cellular necrosis and apoptosis, cytoskeletal damage, diffuse axonal injury, and neuronal degeneration.10,11,16,18,65,92,130 These structural injuries may be the backbone of PTSD as a consequence of MTBI after exposure to blast overpressure waves.3,4,9,10,13,16,17,130 A recent study of the southeastern European regional conflicts by Cernak and colleagues reported the presence of long-term signs and symptoms reflecting a central nervous system disorder in 30% of 665 of patients sustaining blast overpressure.16 In this study pure PTSD was noted in 11% of patients.
TBI is considered to be a strong cause of PTSD and physical health problems among veterans of the Iraq War. A survey of 2525 U.S. soldiers 3 to 4 months after their return from a year-long deployment to Iraq indicated a significant association of PTSD and MTBI. Of these soldiers, 124 (4.9%) reported loss of consciousness and 260 (10.3%) reported altered mental state. Of the soldiers reporting loss of consciousness, 43.9% had PTSD as compared with 27.3% who reported altered mental status. PTSD and depression were important mediators of the relationship between MTBI and poor general health, missed workdays, and medical visits. A similar study of 2235 American veterans by Schneiderman and colleagues showed about 12% with MTBI and 11% with PTSD.5 Other studies have corroborated these findings.1,7–9,16 Further studies are in progress to understand the exact molecular, cellular, and clinical manifestations of blast-induced MTBI and PTSD.4,10
Management
Imaging Studies
Computed Tomography
Injury Profile
Computed tomography (CT), including three-dimensional reconstruction of the head, defines the entry site and trajectory of the fragment into the brain, terminal ballistics (perforating, penetrating, and tangential),66 and involvement of the paranasal sinuses, orbits, skull base, and mastoids. It defines the missile track,21 number of tracks and ricochet,23 whether the penetration is across the midsagittal or midcoronal planes,27 and the presence or absence of intracranial hematomas such as acute epidural, subdural, intracerebral, or intraventricular hematomas.24,27,35,42 The extent of brain edema and ischemia and brainstem involvement is defined by CT (see Fig. 336-5).
Vascular Injury Profile
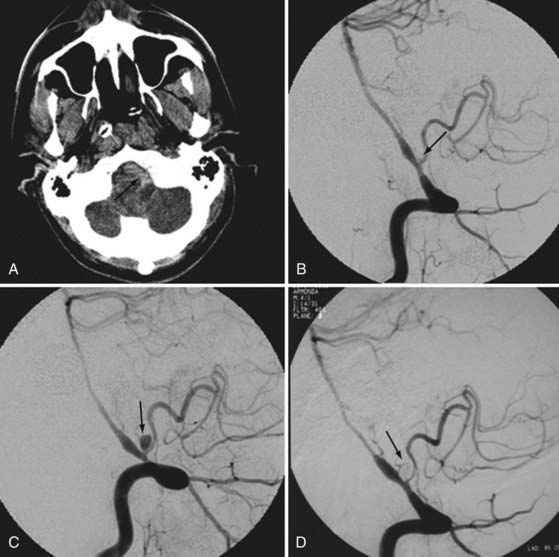
Direct or indirect evidence of vascular injury can clearly be shown by cranial CT. Various degrees of subarachnoid hemorrhage and delayed traumatic intracerebral hematomas can indicate the need for CT or conventional angiography. Patients with pterional and orbitocraniocerebral injuries, fragments associated with acute or delayed intracerebral hematomas, and fragments passing through two dural compartments are specifically prone to harbor TICAs.101,131
Involvement of Air Sinuses and Mastoid Air Cells
Particular attention should be paid to fragments penetrating the paranasal air sinuses and mastoid air cells. These patients are specifically susceptible to leakage of cerebrospinal fluid (CSF) and deep intracranial infections.88,110,132,133
Retained Fragments
There is no question that CT is the best tool for diagnosing retained bone or missile fragments,134–136 especially if the surgery is being performed for minimal débridement.
Deep Infections
During WWII, almost 25% of retained bone fragments were a nidus for deep infections such as abscesses. With the widespread use of antibiotics and proper débridement, the chance of deep central nervous system infection occurring has dropped precipitously; however, for the rare cases of brain abscess attributable to inadequate débridement, the track of the projectile needs to be kept under close scrutiny for several weeks after the missile head wound.110,137–140






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


