Chapter 48 Trigeminal Neuralgia
• Trigeminal neuralgia is a stereotyped, repetitive, unilateral, electric-shock-like facial pain triggered by non-noxious stimulation with clear pain-free intervals. Tic pain is ordinarily spontaneous in onset, but can frequently be triggered by a non-noxious stimulus.
• Continuous pain without a shock-like quality or a cranial nerve deficit raises the suspicion of diseases other than trigeminal neuralgia. Tic douloureux can be caused by any of a number of conditions affecting the ipsilateral trigeminal system. In the vast majority, the cause seems to be compression of the trigeminal nerve at its exit from the pons by an adjacent artery or vein that has elongated and kinked to become wedged against the nerve. In about 1% to 2% of cases, the pain results from a benign tumor in the cerebellopontine angle, and approximately 1% to 8% of patients with trigeminal neuralgia have multiple sclerosis.
• The diagnosis of tic douloureaux is based on the patient’s history of pain as no diagnostic imaging or physiological studies currently available will substitute for the history. Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) have improved the sensitivity and specificity of diagnosing neurovascular compression of the nerve by evaluating the anatomical relationships of the arterial and venous structures with the trigeminal nerve at the root entry zone in the cerebellopontine angle. However, MRI is used primarily as a perioperative adjunct after the clinical diagnosis is made.
• Medical management of tic pain is successful in about 50% of patients and remains the initial approach. The anticonvulsants carbamazepine, phenytoin, and gabapentin appear to be the most effective in controlling the pain of tic douloureux.
• A multimodality approach, including various medical, surgical, or radiosurgical therapies, is most beneficial to patients with tic pain. Gasserian gangliolysis selectively destroys the nocireceptive fibers while preserving the touch fibers. This procedure can be performed using radiofrequency ablation, balloon compression, or glycerol. The success of radiosurgery appears excellent, although long-term recurrence rates are unclear. Of all surgical treatments, microvascular decompression is associated with the lowest rates of recurrence and sensory loss but carries low but significant morbidity rates.
Trigeminal neuralgia, also known as tic douloureux, is an excruciatingly painful condition that is most common in people aged 50 to 70 years. It is a stereotyped, repetitive, unilateral, electric-shock-like facial pain triggered by non-noxious stimulation with clear pain-free intervals.1–5 The incidence of trigeminal neuralgia is 4 to 5 per 100,000 population (median age 67 years).6 It involves the right side of the face more often than the left side, at a ratio of about 3:2. Women are more often affected than men in a ratio that has varied from 2:1 to 4:3 in reported series.7
Etiology and Pathogenesis
Tic douloureux can be caused by any of a number of conditions affecting the ipsilateral trigeminal system. In the vast majority, the cause seems to be compression of the trigeminal nerve at its exit from the pons by an adjacent artery or vein that has elongated and kinked to become wedged against the nerve. In about 1% to 2% of cases, the pain results from a benign tumor in the cerebellopontine angle, such as a meningioma, epidermoid tumor, or acoustic neuroma, or even an arteriovenous malformation.8 Other authors have indicated that 1% to 8% of patients with trigeminal neuralgia have multiple sclerosis.9–13 Very infrequently, trigeminal neuralgia may be the presenting symptom of multiple sclerosis.14 A variety of other rare etiological associations have been reported, but all of these together probably do not account for more than a low percentage of cases. In a significant number of patients, the cause of the tic douloureux is not apparent.
The pathogenesis of trigeminal neuralgia remains uncertain, as are the mechanisms by which treatments are effective. For example, some authors have postulated that nerve root demyelination resulting from neural compression by a blood vessel or tumor or resulting from multiple sclerosis is an important feature, perhaps permitting ephaptic transmission or ectopic impulse generation between adjacent denuded axons. Both peripheral and central mechanisms are most likely required for the production of tic douloureux. Calvin and colleagues presented a comprehensive theory that utilizes two known physiological mechanisms: the trigeminal dorsal root reflex and repetitive firing of extra action potentials from a focal region of altered axonal size or myelination.15 Altered central connectivity and neuronal hyperactivity caused by deafferentation (centralist concept) as well as changes in the trigeminal myelin and axons can lead to altered peripheral sensitivity to chemical and mechanical stimuli (peripheralist concept).15,16 However, as attractive as such ideas are, no theory has yet been postulated that explains all aspects of tic douloureux, such as the pain-free periods, which may last for months or years early in the course of the condition, the triggering of tic pain by non-noxious stimuli, the separation of the trigger areas from the painful region, and the response to anticonvulsants. Elimination of root compression by adjacent vessels does not take into account the effectiveness of numerous other surgical procedures, most of which injure the root or ganglion, but decompression of the root may relieve pain by facilitating remyelination.
Clinical Features
Tic douloureux is diagnosed almost exclusively on the basis of the patient’s history (Box 48.1). The International Headache Society defined trigeminal neuralgia as a “sudden, usually unilateral, severe, brief, stabbing, and recurrent pain in the distribution of one or more branches of the fifth cranial nerve.”17,18 The three divisions of the trigeminal nerve are the ophthalmic, maxillary, and mandibular. For the accurate diagnosis of facial pain, a detailed knowledge of the anatomy of the fifth cranial nerve is essential. By definition, the pain of tic douloureux is confined to the distribution of one trigeminal nerve (Fig. 48.1) and more commonly affects the lower part of the face than the upper.16 The maxillary division of the fifth cranial nerve (V2) is the site of pain alone or in combination with other divisions, most commonly the mandibular division (V3) in 45% of cases. The ophthalmic division (Vl) is least likely to be affected in trigeminal neuralgia (Fig. 48.2). A small number of patients have similar pain syndromes in the territories of the nervus intermedius, glossopharyngeal nerve, or vagus nerve. The pain of untreated tic douloureux occurs unpredictably and is sudden in onset, severe in degree, and short in duration. Often the patient can experience many paroxysms of pain within a single hour, and such bouts may go on for days, with some fluctuation in frequency from hour to hour and day to day. Early in the course of the syndrome, pain-free periods lasting months are common, but as time goes on these natural remissions tend to become less frequent and less prolonged. Although tic pain is ordinarily spontaneous in onset, it can frequently be triggered by a non-noxious stimulus, such as touching the skin on that side of the face, chewing, swallowing, or talking. Some patients are sensitive in certain areas of the face, called trigger zones, which when touched cause an attack of pain. Even a gentle breeze can trigger pain in some patients. The pain has been described as lancinating, lightning-like, or electrical in quality, and has been likened to the pain experienced when a dentist drills into the pulp of a tooth.7 The patient may wince in response to the pain, hence the name tic douloureux. A history of bilateral tic pain can be elicited in 3% of patients, although no patient has bilateral tic pain during one episode.16
BOX 48.1 International Headache Society Criteria for Trigeminal Neuralgia
Paroxysmal attacks of frontal pain last a few seconds to less than 2 minutes.
Pain has at least four of the following characteristics: distribution along one or more divisions of the trigeminal nerve; sudden, intense, sharp, superficial, stabbing or burning in quality; pain intensity severe; precipitation from trigger areas or by certain daily activities such as eating, talking, washing the face or cleaning the teeth; between paroxysms the patient is entirely asymptomatic.
No neurological deficit is found.
Attacks are stereotyped in the individual patient.
Other causes of facial pain are excluded by history, physical examination, and special investigation when necessary.
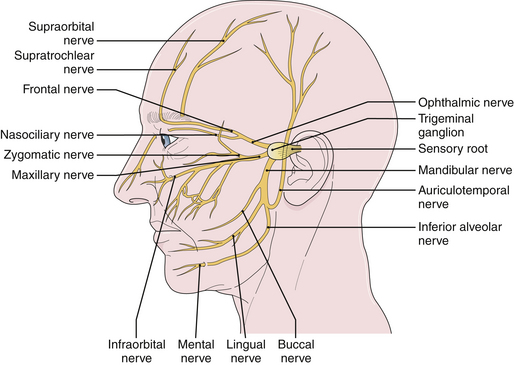
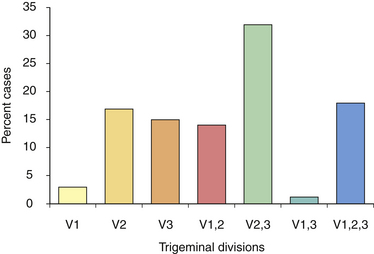
FIGURE 48.2 Distribution of pain among divisions of the trigeminal nerve in patients with tic douloureux
(Data from Loeser J. Tic douloureux. Pain Res Manage 2001;6:156-165.)
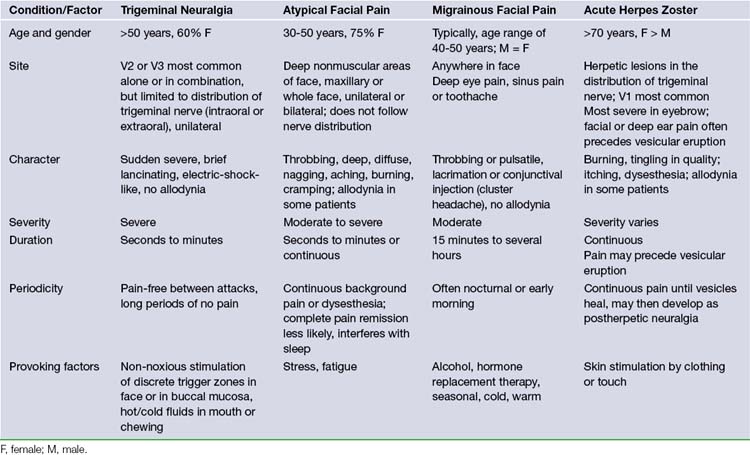
Often the patient who develops tic douloureux sees the dentist first, because lancinating lower facial pain seems to be arising from a certain tooth or teeth. Dentists are often fixated on peripheral lesions as the cause for pain. A diseased tooth in the upper jaw can cause headache on the same side, which may radiate into the orbit or face. A diseased tooth in the lower jaw may cause considerable pain in the distribution of the mandibular division of the nerve, including pain deep in the ear. In addition, dental pain is much more common than tic douloureux. Teeth may be extracted or other dental procedures performed without providing any relief of the pain of tic douloureux. The patient may also consult more than one physician before the correct diagnosis is made. In the majority of patients, the trigeminal neuralgia is idiopathic in that there is no identifiable cause.8 However, the presence of sensory loss mandates a thorough search for structural pathology. Patients with idiopathic trigeminal neuralgia can develop more atypical features with time in the absence of efficacious therapy. In all likelihood, this development coincides with ongoing neuropathic injury. Pain that is continuous, lacks a shock-like quality, or is associated with objective evidence of cranial nerve dysfunction should raise the suspicion of diseases other than idiopathic trigeminal neuralgia. However, the most likely cause of this type of pain is a prior ablative procedure that damages the trigeminal nerve. Atypical facial pain is described as deep, burning, and continual. There is no jabbing onset as occurs in tic douloureux. The pain can radiate behind the ear, down onto the neck, or across to the opposite maxillary area. These patients, in contrast, often clutch their face, unlike the patient with tic douloureux who shields her face but is very careful not to actually touch it (Table 48.1). Myofascial pains involving the muscles of mastication and temporomandibular joint pain occur predominantly in the lateral face. They are also described as aching, burning, or cramping pains, and are often associated with tenderness to palpation of the involved muscles.16
Diagnosis
The diagnosis of tic douloureux is based almost exclusively on the history; as this disease consists only of pain, no diagnostic imaging or physiological studies currently available will substitute for the history. The neurological examination is ordinarily normal except for mild sensory changes in a minority of patients in the region of their pain, with the exception that those few patients with multiple sclerosis or a large structural lesion such as a tumor in the cerebellopontine angle usually have altered trigeminal sensation and other evidence that heralds the underlying disorder. Traditionally, diagnostic radiological studies such as computed tomography or magnetic resonance imaging have been normal in the usual patient with tic douloureux, but they have been performed to identify the exceptional patient with a recognizable etiological condition such as those just mentioned.7 Patients with a Chiari malformation may also develop trigeminal neuralgia, thought to be the result of venous or arterial compression of the cranial nerves along with the tonsillar ectopia. Recent advances in magnetic resonance imaging and magnetic resonance angiography have improved the sensitivity and specificity of diagnosing neurovascular compression of the nerve by evaluating the anatomical relationships of the arterial and venous structures with the trigeminal nerve at the root entry zone in the cerebellopontine angle.16 However, so far these studies have been more used as a preoperative adjunct than for diagnostic purposes.19,20 Continued development of MRI is likely to lead to the ability to discern if there is a vascular impingement on the nerve and thereby may influence choice of treatment.
Related posts:
 Cavernous Malformations Management Strategies
Cavernous Malformations Management Strategies
 Stereotactic Radiosurgery of Vascular Malformations
Stereotactic Radiosurgery of Vascular Malformations
 Spasticity: Classification, Diagnosis, and Management
Spasticity: Classification, Diagnosis, and Management
 Application of Current Radiation Delivery Systems and Radiobiology
Application of Current Radiation Delivery Systems and Radiobiology
 Spinal Dysraphism and Tethered Spinal Cord
Spinal Dysraphism and Tethered Spinal Cord
 Pituitary Tumors: Diagnosis and Management
Pituitary Tumors: Diagnosis and Management



