Fig. 39.1
Triple H-associated posterior reversible encephalopathy syndrome. Axial CT image (a) shows scattered subarachnoid hemorrhage. Follow-up MRI (b–d) shows bilateral posterior cerebral hemisphere cortical and subcortical vasogenic edema
39.4 Differential Diagnosis
The main differential consideration for new neurological deficits following subarachnoid hemorrhage is vasospasm-associated ischemia (Fig. 39.2). Although infarction secondary to vasospasm and posterior reversible encephalopathy can both appear as bilateral hypoattenuating foci on CT, infarcts typically demonstrate perfusion deficits, while posterior reversible encephalopathy tends to show elevated perfusion. Diffusion-weighted imaging can also be useful for characterizing these lesions, whereby acute infarcts display restricted diffusion, while posterior reversible encephalopathy more commonly demonstrates elevated diffusivity.
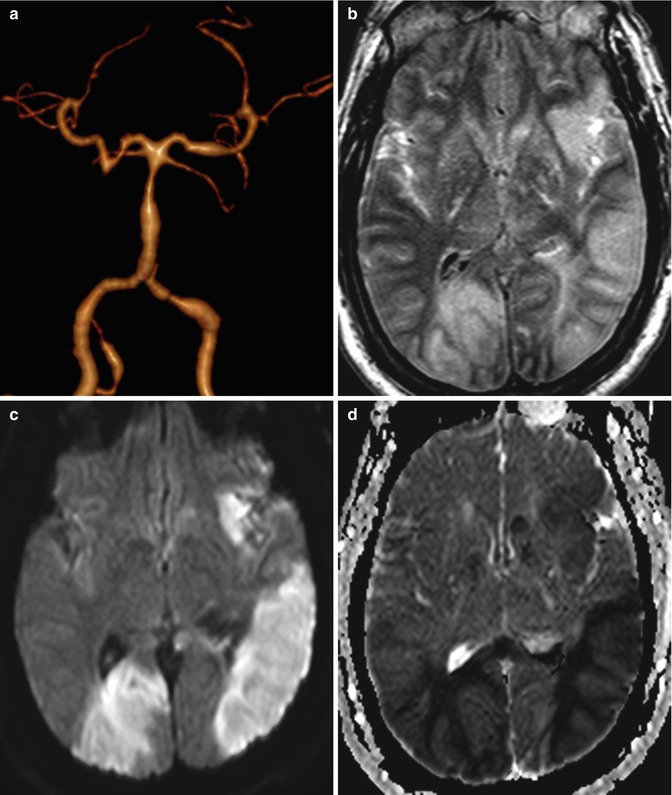
Fig. 39.2




Infarct related to vasospasm after subarachnoid hemorrhage. Posterior circulation 3-D reformatted CTA image (a) shows multiple stenotic lesions. Axial FLAIR (b), DWI (c), and ADC map (d) show that acute infarcts predominantly affect the posterior hemispheres bilaterally
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
