CHAPTER 12
Vascular Supply of the Brain
The brain and spinal cord are critically dependent on an uninterrupted supply of oxygenated blood, and thus are dependent on unimpeded flow through the cerebral vessels. About 18% of the total blood volume in the body circulates in the brain, which accounts for about 2% of the body weight. The blood transports oxygen, nutrients, and other substances necessary for proper functioning of the brain and carries away metabolites. Loss of consciousness occurs in less than 15 seconds after blood flow to the brain has stopped, and irreparable damage to the brain tissue occurs within 5 minutes.
Cerebrovascular disease, or stroke, occurs as a result of vascular compromise or hemorrhage and is one of the most frequent sources of neurologic disability. Because the cerebral vessels each tend to irrigate specific territories in the brain, their occlusion results in highly stereotyped syndromes that, even prior to imaging studies, can suggest the site of the vascular lesion.
Nearly half of the admissions to many busy neurologic services are because of strokes. Cerebrovascular disease is the third most common cause of death in industrialized societies. Because thrombolysis—if accomplished in the initial hours after a stroke occurs—can sometimes restore blood flow and improve clinical status, early recognition and treatment of stroke are essential.
ARTERIAL SUPPLY OF THE BRAIN
Circle of Willis
The circle of Willis (named after the English neuroanatomist Sir Thomas Willis) is a hexagon of vessels that gives rise to all of the major cerebral arteries. It is fed by the paired internal carotid arteries and the basilar artery. When the circle is complete, it contains a posterior communicating artery on each side and an anterior communicating artery. The circle of Willis shows many variations among individuals. The posterior communicating arteries may be large on one or both sides (embryonic type); the posterior cerebral artery may be thin in its first stretch (embryonic type); and the anterior communicating artery may be absent, double, or thin. Despite these variations, occlusion of each of the major cerebral arteries usually produces a characteristic clinical picture.
Characteristics of the Cerebral Arteries
The course of the large arteries (at least in their initial stretches) is largely ventral to the brain in a relatively small region. The arteries course in the subarachnoid space, often for a considerable distance, before entering the brain itself; rupture of a vessel (eg, from an aneurysm that has burst) tends to cause a subarachnoid hemorrhage.
Each major artery supplies a certain territory, separated by border zones (watershed areas) from other territories; sudden occlusion in a vessel affects its territory immediately, sometimes irreversibly.
Principal Arteries
The arterial blood for the brain enters the cranial cavity by way of two pairs of large vessels (Figs 12–1 and 12–2): the internal carotid arteries, which branch off the common carotids, and the vertebral arteries, which arise from the subclavian arteries. The vertebral arterial system supplies the brain stem, cerebellum, occipital lobe, and parts of the thalamus, and the carotids normally supply the remainder of the forebrain. The carotids are interconnected via the anterior cerebral arteries and the anterior communicating artery; the carotids are also connected to the posterior cerebral arteries of the vertebral system by way of two posterior communicating arteries, part of the circle of Willis.
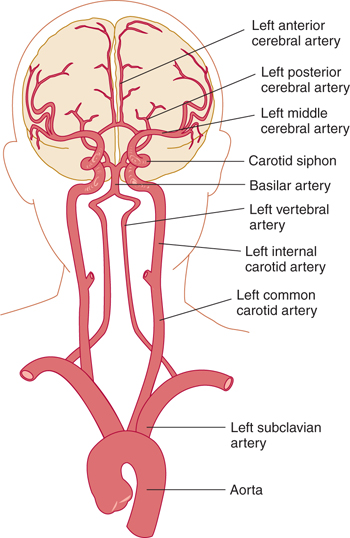
FIGURE 12–1 Major cerebral arteries.
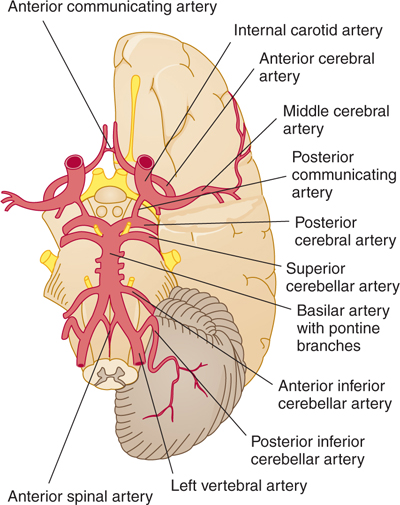
FIGURE 12–2 Circle of Willis and principal arteries of the brain stem.
Vertebrobasilar Territory
After passing through the foramen magnum in the base of the skull, the two vertebral arteries form a single major midline vessel, the basilar artery (Figs 12–2 and 12–3; see also Fig 7–10). This vessel terminates in the interpeduncular cistern in a bifurcation as the left and right posterior cerebral arteries. These may be thin, large, or asymmetric depending on retention of the embryonic pattern (in which the carotid supplies the posterior cerebral arteries).
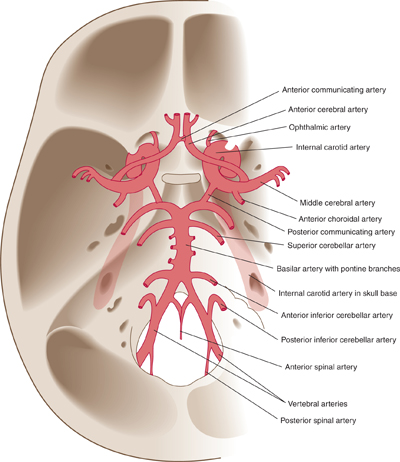
FIGURE 12–3 Principal arteries on the floor of the cranial cavity (brain removed).
Several pairs of small circumferential arteries arise from the vertebral arteries and their fused continuation, the basilar artery. These are the posterior and anterior inferior cerebellar arteries, the superior cerebellar arteries, and several smaller branches, such as the pontine and internal auditory arteries. These arteries can show asymmetry and variability but, in general, they irrigate critically important parts of the brain. The small penetrating arteries, which branch off the basilar artery, supply vital centers in the brain stem (Fig 12–4).
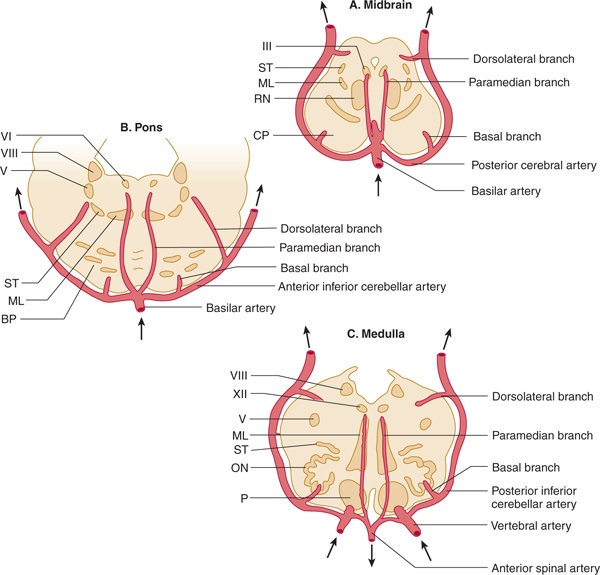
FIGURE 12–4 Arterial supply of the brain stem. A: Midbrain. The basilar artery gives off paramedian branches that supply the oculomotor (III) nerve nucleus and the red nucleus (RN). A larger branch, the posterior cerebral artery, courses laterally around the midbrain, giving off a basal branch that supplies the cerebral peduncle (CP) and a dorsolateral branch supplying the spinothalamic tract (ST), medial lemniscus (ML), and superior cerebellar peduncle. The posterior cerebral artery continues (upper arrows) to supply the thalamus, occipital lobe, and medial temporal lobe. B: Pons. Paramedian branches of the basilar artery supply the abducens (VI) nucleus and the medial lemniscus (ML). The anterior inferior cerebellar artery gives off a basal branch to the descending motor pathways in the basis pontis (BP) and a dorsolateral branch to the trigeminal (V) nucleus, the vestibular (VIII) nucleus, and the spinothalamic tract (ST) before passing to the cerebellum (upper arrows). C: Medulla. Paramedian branches of the vertebral arteries supply descending motor pathways in the pyramid (P), the medial lemniscus (ML), and the hypoglossal (XII) nucleus. Another vertebral branch, the posterior inferior cerebellar artery, gives off a basal branch to the olivary nuclei (ON) and a dorsolateral branch that supplies the trigeminal (V) nucleus, the vestibular (VIII) nucleus, and the spinothalamic tract (ST) on its way to the cerebellum (upper arrows). (Reproduced, with permission, from Simon RP, Aminoff MJ, Greenberg DA: Clinical Neurology, 4th ed. Appleton & Lange, 1999.)
Carotid Territory
The internal carotid artery passes through the carotid canal of the skull and then curves forward within the cavernous sinus and up and backward through the dura, forming the carotid siphon before reaching the brain (see Fig 12–1). The first branch is usually the ophthalmic artery. In addition to their links with the vertebral system, the carotids branch into a large middle and a smaller anterior cerebral artery on each side (Fig 12–5). The two anterior cerebral arteries usually meet over a short distance in midplane to form a short but functionally important anterior communicating artery. This vessel forms an anastomosis between the left and right hemispheres, which is especially important when one internal carotid becomes occluded. The anterior choroidal artery, directly off the internal carotid, carries blood to the choroid plexus of the lateral ventricles as well as to adjacent brain structures.
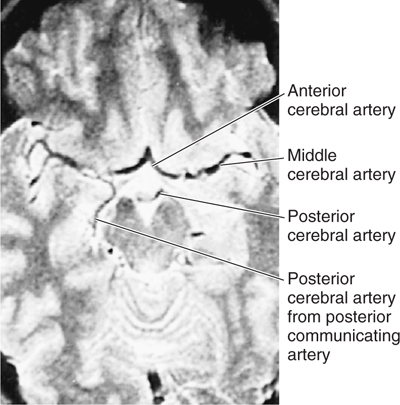
FIGURE 12–5 Magnetic resonance image of a horizontal section at the level of the circle of Willis.
Cortical Supply
The middle cerebral artery supplies many deep structures and much of the lateral aspect of the cerebrum; it breaks up into several large branches that course in the depth of the lateral fissure, over the insula, before reaching the convexity of the hemisphere. Because it supplies cortical areas essential for speech in the left hemisphere, the left middle cerebral artery is sometimes called the “artery of speech”. The anterior cerebral artery and its branches course around the genu of the corpus callosum to supply the anterior frontal lobe and the medial aspect of the hemisphere; they extend quite far to the rear. The posterior cerebral artery curves around the brain stem, supplying mainly the occipital lobe and the choroid plexuses of the third and lateral ventricles and the lower surface of the temporal lobe (Figs 12–6 and 12–7).
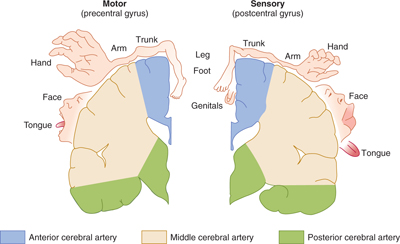
FIGURE 12–6 Arterial supply of the primary motor and sensory cortex (coronal view). Notice the location of the homunculus with respect to the territories of the cerebral arteries. (Reproduced, with permission, from Simon RP, Aminoff MJ, Greenberg DA: Clinical Neurology, 4th ed. Appleton & Lange, 1999.)
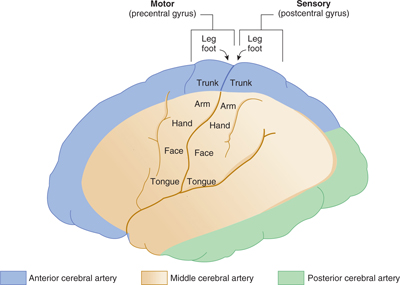
FIGURE 12–7 Arterial supply of the primary motor and sensory cortex (lateral view). (Reproduced, with permission, from Simon RP, Aminoff MJ, Greenberg DA: Clinical Neurology, 4th ed. Appleton & Lange, 1999.)
By comparing the territories irrigated by the anterior, middle, and posterior cerebral arteries on the one hand and the homunculus on the other, the student can predict the deficits caused by a stroke affecting the territories irrigated by each of these arteries (see Fig 12–6):
In a stroke affecting the territory of the middle cerebral artery, weakness and sensory loss are most severe in the contralateral face and arm, but the leg may be only mildly affected or unaffected.
In contrast, in a stroke affecting the territory irrigated by the anterior cerebral artery, weakness is most pronounced in the contralateral leg.
Cerebral Blood Flow and Autoregulation
Many physiologic and pathologic factors can affect the blood flow in the arteries and veins of the brain. Under normal conditions of autonomic regulation, the pressure in the small cerebral arteries is maintained at 450 mm H2O. This ensures adequate perfusion of the cerebral capillary beds despite changes in systemic blood pressure. Increased activity in one cortical area is accompanied by a shift in blood volume to that area.
VENOUS DRAINAGE
Types of Channels
The venous drainage of the brain and coverings includes the veins of the brain itself, the dural venous sinuses, the dura’s meningeal veins, and the diploic veins between the tables of the skull (Figs 12–8 to 12–10). Emissary veins drain from the scalp, through the skull, into the larger meningeal veins and dural sinuses. Communication exists between most of these channels. Unlike systemic veins, cerebral veins have no valves and seldom accompany the corresponding cerebral arteries.
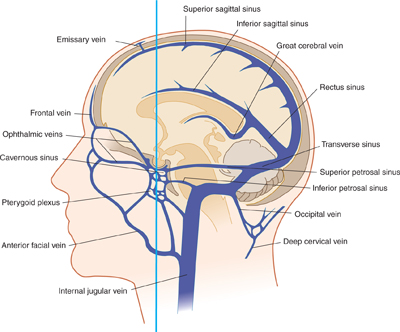
FIGURE 12–8 Organization of veins and sinuses of the brain. Figure 12–11 provides a frontal view, cut along the plane shown by the vertical line.
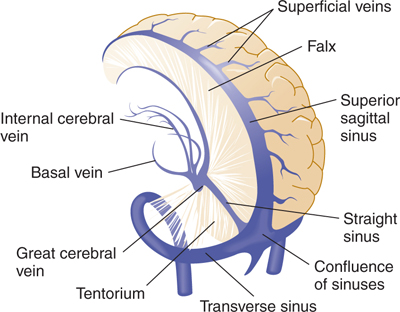
FIGURE 12–9 Three-dimensional view of veins and sinuses of the brain, left posterior lateral view.
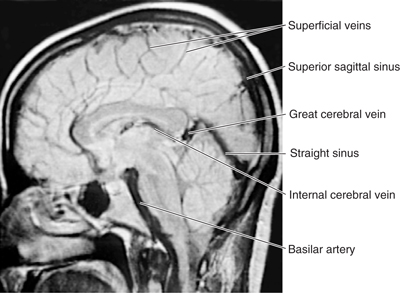
FIGURE 12–10 Magnetic resonance image of a midsagittal section through the head showing venous channels.
Internal Drainage
The interior of the cerebrum drains into the single midline great cerebral vein (of Galen), which lies beneath the splenium of the corpus callosum. The internal cerebral veins (with their tributaries, the septal, thalamostriate, and choroidal veins) empty into this vein, as do the basal veins (of Rosenthal), which wind (one right and one left) around the side of the midbrain, draining the base of the forebrain. The precentral vein from the cerebellum and veins from the upper brain stem also empty into the great vein, which turns upward behind the splenium and joins the inferior sagittal sinus to form the straight sinus. The venous drainage of the base of the cerebrum is also into the deep middle cerebral vein (coursing in the lateral fissure) and then to the cavernous sinus.
Cortical Veins
Venous drainage of the brain surface is generally into the nearest large vein or sinus, from there to the confluence of the sinuses, and ultimately to the internal jugular vein (see Fig 12–8).
The veins of the cerebral convex surfaces are divided into superior and inferior groups. The 6 to 12 superior cerebral veins run upward on the hemisphere’s surface to the superior sagittal sinus, generally passing under any lateral lacunae. Most of the inferior cerebral veins end in the superficial middle cerebral vein. The inferior cerebral veins that do not end in this fashion terminate in the transverse sinus. Anastomotic veins can be found; these connect the deep middle cerebral vein with the superior sagittal sinus or transverse sinus.
Venous Sinuses
Venous channels lined by mesothelium lie between the inner and outer layers of the dura; they are called intradural (or dural) sinuses. Their tributaries come mostly from the neighboring brain substance. All sinuses ultimately drain into the internal jugular veins or pterygoid plexus. The sinuses may also communicate with extracranial veins via the emissary veins. These latter veins are important for two reasons: The blood can flow through them in either direction, and infections of the scalp may extend by this route into the intracranial structures.
Of the venous sinuses, the following are considered most important:
Superior sagittal sinus: between the falx and the inside of the skull cap.
Inferior sagittal sinus: in the free edge of the falx.
Straight sinus: in the seam between the falx and the tentorium.
Transverse sinuses: between the tentorium and its attachment on the skull cap.
Sigmoid sinuses: S-curved continuations of the transverse sinuses into the jugular veins; a transverse and a sigmoid sinus together form a lateral sinus.
Sphenoparietal sinuses: drain the deep middle cerebral veins into the cavernous sinuses.
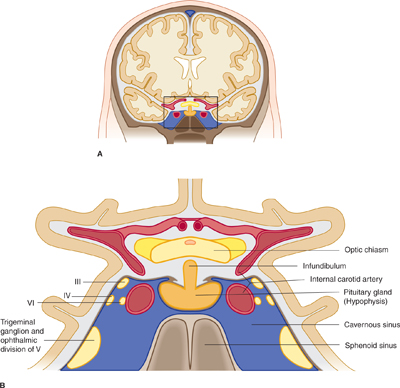
Cavernous sinuses: on either side of the sella turcica. The cavernous sinuses receive drainage from multiple sources, including the ophthalmic and facial veins. Blood leaves the cavernous sinuses via the petrosal sinuses (see Fig 12–8). The cavernous sinuses are convoluted, with different chambers separated by fibrous trabeculae; thus, they have the appearance of a cavern. A number of important arteries and cranial nerves are embedded within the cavernous sinus and its walls. The internal carotid artery runs through the cavernous sinus (Fig 12–11). In addition, the oculomotor, trochlear, and abducens nerves run through the cavernous sinus, as does the ophthalmic division of the trigeminal nerve, together with the trigeminal ganglion.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


