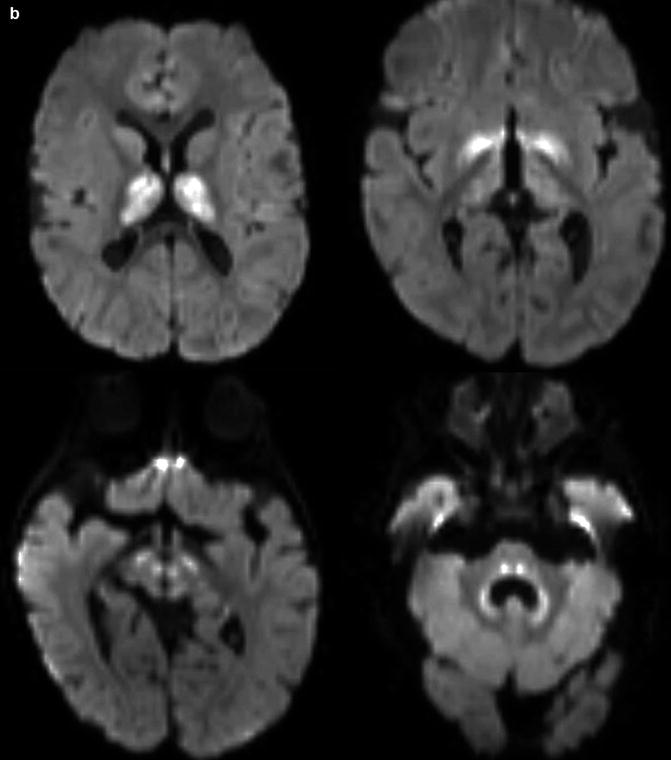
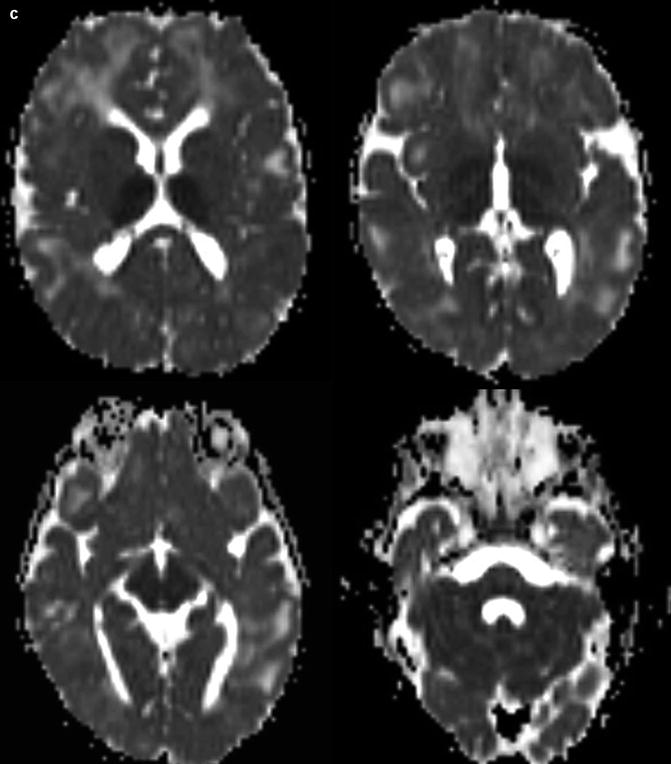
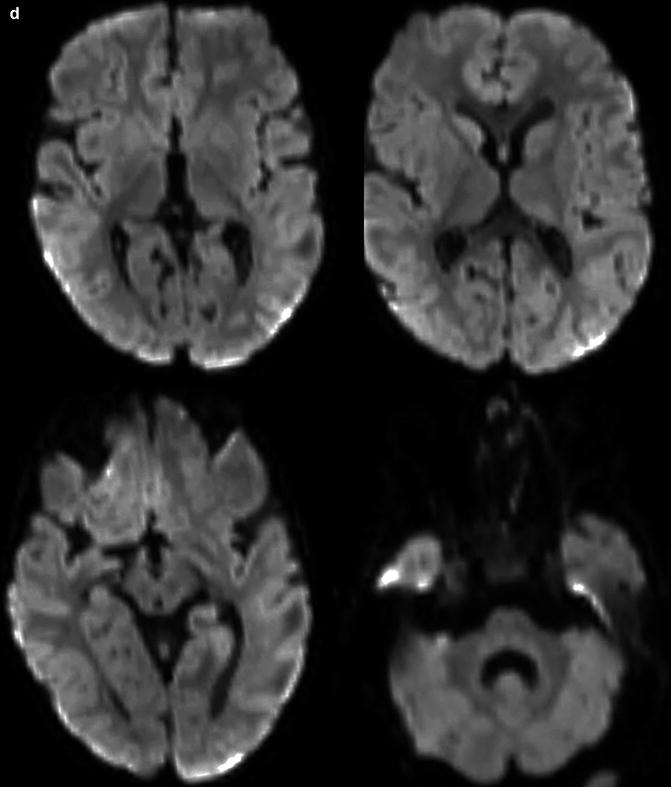
Fig. 29.1
Vigabatrin neurotoxicity. An infant with a history of tuberous sclerosis treated with vigabatrin presented with lethargy. Axial T2-weighted MR images (panel a), DWI (panel b), and ADC maps (panel c) show bilateral symmetric T2 hyperintensity and restricted diffusion within the thalami, basal ganglia, midbrain, and dentate nuclei. The abnormalities resolved within 2 months after cessation of vigabatrin (panel d)
29.4 Differential Diagnosis
The diagnosis of vigabatrin neurotoxicity should be straightforward in an infant with the described imaging findings and treatment history. Nevertheless, possible differential considerations by anatomic location include the following (many of these conditions can affect multiple anatomical sites):
Get Clinical Tree app for offline access

Bilateral basal ganglia T2 hyperintensity: Hypoxic-ischemic injury, viral encephalitis, deep cerebral vein thrombosis, glutaric aciduria type 1, biotin-responsive encephalopathy, neurofibromatosis type 1 (Fig. 29.2), and mitochondrial encephalopathies
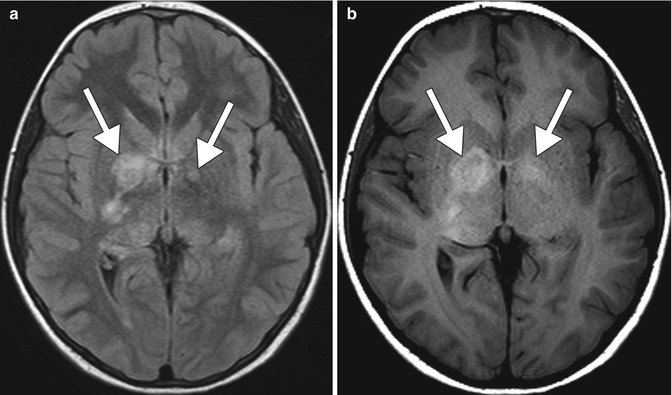
Fig. 29.2
Neurofibromatosis type 1. Axial FLAIR MRI (a) shows patchy hyperintensity in the bilateral basal ganglia, right greater than left (arrows). The corresponding axial T1-weighted MRI (b) shows corresponding T1 hyperintensity in the basal ganglia (arrows)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







