(1)
Department of Neurosurgery, St Elisabeth-Tweesteden Hospital, Tilburg, The Netherlands
Roughly a decade after Broca published his findings on the left frontal speech area, in 1874 Carl Wernicke (1848–1905) published a now famous monograph on different clinical forms of aphasia, The Symptom Complex of Aphasia: A Psychological Study on an Anatomical Basis (German: Der aphasische Symptomencomplex: Eine Psychologische Studie auf Anatomischer Basis) [1]. Wernicke is particularly remembered for his description of sensory aphasia and for his wiring diagram that eventually grew to become the classical language model in neurology. He noted that patients with a lesion of the left temporal lobe had comprehension difficulties but, as opposed to Broca’s aphasics, had fluent speech with a relatively intact vocabulary. As in the case of Broca, the temporal language area was eventually named after Wernicke in honour of his discovery. The posterior part of the superior temporal gyrus is generally considered the core of Wernicke’s area, but the area itself has always remained poorly defined in anatomical terms. Wernicke was not the first to write about aphasia with comprehension disorders. Bastian (1869) and Schmidt (1871) did before him, but they did not provide autopsy results or any underlying anatomical framework, and their papers failed to gain the attention of the medical community [2–4].
From what one reads about Wernicke in medical textbooks or on the Internet, it is easy to get the impression that he, like Broca, was a strict localist and that their two language areas nicely complement each other and form a comprehensive and complete language model: Broca’s area for the productive/motor part of language and Wernicke’s area for the receptive/sensory part of it. However, Wernicke did not plead for strict localization of function to one area; he was in fact one of the first ‘connectionists’, holding that multiple areas are necessary in the orchestration of a given brain function. He himself wrote in 1874 that:
only the most elementary psychic functions can be assigned to defined areas of the cortex [examples are given of visual, olfactory and tactile perception] (…) Everything that goes beyond these simplest functions, the association of different impressions into a concept, thinking, consciousness, is an achievement of the fiber tracts which connect the different regions of the cortex to each other, the so-called association system of Meynert [1].
2.1 Meynert
Wernicke was not the first to suggest such ideas. Most of the credit is probably due to Theodor Meynert (1833–1892), Wernicke’s teacher in neuroanatomy, who made several important contributions and improved histological methods to study the structure and function of the connecting fibre systems [5]. Wernicke repeatedly acknowledges Meynert, for instance, at the beginning of his 1874 monograph: ‘the theory put forward here follows almost automatically from the study of Meynert’s writings and dissections’ [1]. Although the first descriptions of fibre bundles date back to Vicq d’Azyr (1786) and Gall (1810), Meynert described them in detail and differentiated between projection fibres (connecting cortical areas to subcortical parts of the brain) and association fibres (interconnecting cortical areas) [6]. By following the tracts, he was able to deduce that the posterior part of the brain (posterior to the central sulcus) was ‘sensory’ in function and the anterior part ‘motor’. Wernicke adopted the sensorimotor division of Meynert, although he was unsure of the nature of the parietal lobe which he described as an intermediate area of still conflicting functions.1 Meynert had also published an important work in which he demonstrated that the auditory fibres terminated in the cortex of the Sylvian fissure, and he assumed this area to be a ‘sound-field’ (German: Klangfeld) [7]. This view was supported by autopsy findings of lesions in the insular and the perisylvian region. Eminent authors and aphasiologists have suggested that Meynert’s historical role has been underestimated [8]. Geschwind wrote in 1974 that:
the significance of Meynert’s contribution to the study of aphasia has generally been overlooked. In the discussions of the history of aphasia that I have so far consulted, he is mentioned only as Wernicke’s teacher. (…) It is important to appreciate that it was apparently he who first convincingly showed that aphasia could occur in temporal lobe lesions. It was Wernicke’s function to complete the cycle started by Meynert by showing how this fact achieved meaning in terms of Meynert’s own studies of the brain, and to point out the important fact that this new localization corresponded to a clinical picture different from that seen in lesions of Broca’s area [9].
Wernicke wrote his monograph when he was just 26. It was his first work on aphasia and also the one that became his most well known. In particular, his concepts of clinical aphasia and his connectionist thinking made a lasting impact and are still the subject of lively debate. Wernicke made several other important contributions in the field of neurology and psychiatry, but it is not widely known that he continued writing and reviewing articles on aphasia and that he refined and even changed some of his opinions in later works. The basis of his work on aphasia was clearly laid in his monograph, however, and therefore I will describe it in more detail in the rest of this chapter.
2.2 The Symptom Complex of Aphasia, Part I
Wernicke’s monograph consists of three parts. In the first part (pp. 3–12), a general theory is formulated for the representation of cognitive functions in the brain. Wernicke introduces a scheme that is the basis for all of his language models and is in its most elementary form a ‘reflex arc’ (see Fig. 2.1). In this model, any sensory stimulus (E, Empfindung) is able to leave a memory image (O, Erinnerungsbild or Empfindungsrest) in the sensory part of the brain. Wernicke assumed that ‘molecular changes’ in brain cells then consolidate the effects of the brief peripheral stimuli [1]. Bodily movements or changes in musculature leave memory images in a similar manner. These are termed movement images (F, Bewegungsbild) and are located in the motor (anterior) part of the brain. Sensory and motor images are connected by associative fibre systems of which the strength of the connections is variable. Wernicke speaks of ‘resistance’ that is ‘lowered’ once a trajectory is used more often [1]. This resembles the Hebbian principles that were only to be formulated in the middle of the twentieth century. Wernicke’s model also resembles the contemporary view on brain functional organization [10]. Take, in an example from his later work, the way in which Wernicke describes the representation of an object, a bell:

Fig. 2.1
Wernicke’s elementary scheme to explain the representation of cognitive functions in the brain. Any sensory stimulus (E, Empfindung) can leave a memory image (O, Erinnerungsbild or Empfindungsrest) in the sensory part of the brain. Movement images (F, Bewegungsbild) are in a similar manner represented in the anterior part of the brain and subsequently can lead to movements (B, Bewegung). The ‘reflex arc’ is completed by (variable) interconnections between sensory and motor areas (OF) (Figure taken from Wernicke, 1874 [1])
The memory images of a bell (…) are deposited in the cortex and located according to the sensory organs. These would then include the acoustic imagery aroused by a bell, visual imagery established by means of form and color, tactile imagery acquired by cutaneous sensation, and finally, motor imagery as gained by exploratory movements of the fingers and the eyes.2
A concept thus arises when different brain areas work in unison. The ‘knowledge’ of any object (made up by the combined properties of it) is thereby distributed over a number of brain areas and is thus not strictly localized. Because all different functional units are interconnected, it is possible to activate the entire ‘network’ by activation of part of it. Again quoting Wernicke from the paper of Gage and Hickok (2005):
Close association between these various memory images has been established by repeated experience of the essential features of bells. As a final result, arousal of each individual image is adequate for awakening of the concept as a whole. In this way a functional unit is achieved. Such units form the concept of the object, in this case a bell.
Any movement image is linked to multiple interconnected memory images that can have different locations in the brain. Vice versa, there is usually more than one movement image ‘active’ (German: gemeinschaftlich ins Bewusstsein gerufen) [1]. Wernicke thus describes a functional topography that is much more complex than is shown in his illustrations. Cognitive functions were to him represented in mosaic-like association systems. The figures that are depicted in his monograph were intended as schematic illustrations to make his point; Wernicke himself referred to them as ‘schemes’ [12]. Unfortunately, these illustrations have been interpreted far too literally in the history of neuroscience and neurology. It is certainly ironic that Wernicke’s language model has been used to advocate a strict localist view on language representation, whereas Wernicke himself had a different and much more sophisticated vision. His illustrations deliberately lack detailed anatomical information, as anyone familiar with Wernicke’s work will agree. Wernicke devoted a large part of his scientific career to the study of anatomy and neuropathology and was well trained in anatomical dissections. In his 1874 monograph, for instance, he describes stepwise dissection of the temporal lobe and insula. Figure 2.2 shows some of the illustrations from a paper on comparative anatomy he published just 2 years later, when he was still a resident in the Charité in Berlin. It is of interest, although maybe only from a historical point of view, to quote from the introduction of this 1876 paper where Wernicke still somehow seems to doubt the location of the language centre:
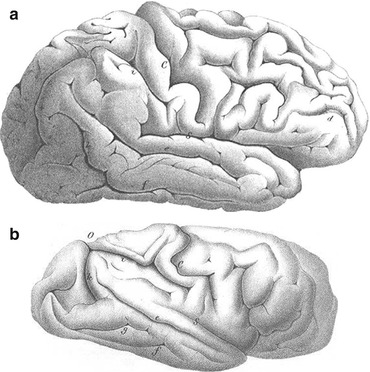
Fig. 2.2
Drawings of the brain of a human (top) and a chimpanzee (not to scale) (Figures taken from Wernicke’s The Primitive Convolution of the Human Brain, 1876 [13])
In recent times, evidence has been presented for the fact that certain functions are bound to certain convolutions or regions. There is no doubt that the first frontal gyrus is the centre for speech movements; it is also likely that the first temporal gyrus is a sensory speech area [13].
In the period 1897–1903, Wernicke published the three-part Atlas des Gehirns (brain atlas), together with other eminent authors such as Foerster. The atlas included myelin-stained sections of the brain in coronal, axial and sagittal planes [14]. Wernicke identified several fasciculi, some of which were named after him [6]. Wernicke was convinced that anatomical development and architecture needed to be studied in order to identify normal from abnormal brains and to understand the neural basis of higher cortical functions. He rejected the idea that the convolutional pattern was random or circumstantial.
2.3 The Symptom Complex of Aphasia, Part II
In the second part of the monograph (pp. 12–38), Wernicke describes his theory of aphasia by giving a detailed description of the clinical profiles that result from lesions at five different locations in the psychic reflex arc of his language model (shown in Fig. 2.3A):

Fig. 2.3
Four different schemes that Wernicke used to explain his theory of aphasia, taken from his 1874 monograph. For unknown reasons these schemes are projected on the right hemisphere. The structure of the schematic brains is similar in all cases, showing three frontal and three temporal convolutions. The central sulcus (C) separates the precentral and postcentral convolution. Parietal and occipital regions are not shown in any detail. Note that the memory areas differ in location between the various models. (Top left, A) This is the well-known figure from medical textbooks that essentially forms the basis of classical neurological language models. α is the acoustic nerve that in part terminates in the temporal sensory language area. This area (a) is connected to the frontal motor language area (b). (Top right, B) The model has been expanded with memory areas for tactile (c) and optical (d) images. ‘Knowledge’ of objects or words is diffusely stored in the network that is formed by areas a, c and d. Wernicke is not very specific on locations for these tactile and optical areas, other than that the optical memory areas are located in the posterior parts of the brain. Note also that area a has a different location within the various figures. (Bottom left, C) Specific areas for reading (α) and writing (β) have been added. Wernicke postulated that connections αβ and ab in reality have an intimate anatomical relationship (not clear from the model). (Bottom right, D) Language model in subjects that are born deaf-mute, but who were able to acquire speech. According to Wernicke, this proves that there must exist direct connections from tactile (c) and optical (o) areas to the motor speech area b. In deaf-mute subjects, areas c and d form the first part of the ‘reflex arc’ (Figures taken from Wernicke, 1874 [1])
Any interruption of the pathway aal bbl can cause aphasia. The clinical picture will however vary according to the portion of the path affected by the interruption [1].
This essentially forms the foundation of what became the classical neurological model of aphasia. It also set the framework for research on aphasia for at least the first half of the twentieth century. However, when Wernicke’s doctoral thesis and his later work is read carefully, it becomes clear that he describes a much more modern view on language representation and organization than he is usually credited and remembered for. The rest of this section will be structured according to the five different lesions that Wernicke described and the subsequent research on each.
2.3.1 Lesion of the Acoustic Nerve
A lesion of the afferent tract to a (acoustic nerve) will lead to deafness without aphasia, but only, Wernicke writes, if language has already been learned. Children need the auditory input to be able to form auditory memory images. In a first phase, they acquire the words by repeating them. ‘Begriff’ arises in a later phase, when the word itself has already been mastered. Wernicke asks himself what would happen when a child is deaf in the right ear but still has a normal language development. Assuming that the right acoustic nerve terminates in the left hemisphere, and vice versa (although Wernicke explicitly states that this was still unsure at the time), he hypothesizes that in this case the right temporal lobe shall have the potential to acquire language functions. At a later part in his monograph, Wernicke elaborates on this in a more general manner and states that language is normally a function of the left hemisphere, but that the right hemisphere can take over language functions in case of left hemisphere pathology. In fact, in many of the case reports that are listed in the third part of his monograph, Wernicke describes recovery of aphasic symptoms over time. He thereby repeatedly describes a phenomenon that we now would call ‘brain plasticity’. Similar suggestions were also made by Broca.
In the course of the illness the other hemisphere could have taken over the function of the left temporal lobe, as indeed takes place very rapidly in sensory aphasia [1].
2.3.2 Lesion of the Auditory Memory Centre: ‘Wernicke’s Aphasia’
A lesion of the centre for auditory images (area a) will lead to ‘sensory aphasia’. The resulting symptom complex later became known as Wernicke’s aphasia, although Wernicke’s own description is significantly different from some later definitions. The most important symptom of sensory aphasia, according to Wernicke, is that ‘language is not understood, but hearing is demonstrably preserved’ [12]. Words will be heard as meaningless noise [15]. The vocabulary is largely intact, but there is a ‘confusion of words’ [German: Verwechslungen der Wörter]. The term ‘paraphasia’ was not yet used and was later introduced by Kussmaul in 1877 [16]. According to Wernicke, the explanation for these (mild) speech problems is a defective mechanism via route ab. This prevents an unconscious correction of what has been spoken.
It seems that during normal speech the sound image [Klangbild] is always unconsciously innervated, as is easily understandable in terms of the genesis of language. The sound image is simultaneously hallucinated, as it were, and therefore able to continuously correct the execution of movements [Bewegungsvorstellungen] [1].
Wernicke explains why patients are not deaf when area a is lesioned, and he does so by assuming that the acoustic nerve disperses over a wider area of the brain than just area a (again demonstrating that Wernicke’s illustrations are only simplified schemes).
Thus that part of the central projection of the acoustic nerve which contains word sounds [Wortklänge] may be destroyed while all noises or all musical tones may still be perceived [1].
Next, Wernicke explains in more detail what happens when area a is lesioned:
If area a1, the cortex of the first temporal convolution, is destroyed, the sound images [Klangbilder] of the names of all possible objects will be extinguished from memory, although the concepts may still remain in their full clarity. For in most cases the sound image is of secondary importance for the concept of the object, whereas the somaesthetic sense images [Gefüls- und Tastsinnsbilder] are of critical importance for it [1].
When I first read this passage, I had difficulty understanding it, because I had never really thought about the difference between hearing a word and truly understanding its meaning. Just hearing a word does not necessarily imply that you grasp its meaning. Take, as an example, listening to pseudowords, e.g. vonk or bhutap. These words conform to phonological conventions (i.e. they sound like real words) but have no meaning. Therefore, these pseudowords do not trigger the associations in the brain network that normally lead to an understanding of an underlying meaning or concept. So Wernicke’s auditory area a is needed to hear the words, but is more or less redundant for comprehension [Begriff] because this will only arise when several different memory areas are conjointly activated. Wernicke uses several illustrations (Fig. 2.3B) to visualize this concept and is now able to explain why destruction of one sensory memory area does not lead to a loss of understanding of the concept as a whole, as auditory memory images (a) are connected to associated tactile images (c) and optical images (d).All three sensory modalities also conjointly determine which word is eventually selected by means of a weighed contribution of their inputs to area b. If one of the sensory areas is lesioned, ‘innervation’ of motor speech centre b is determined by the sum of the remaining other areas. This is fundamentally different to the classical interpretation of the model in Fig. 2.3A, whereby a lesion of area a would deprive area b of any input. Due to a parallel design, the system has inbuilt redundancies and is able to keep functioning despite a lesion of one of its subcomponents. Note that each sensory area has a similar architecture and itself consists of multiple interconnected areas. This is why Wernicke can speak of a ‘partial’ lesion of a particular sensory language centre, whereby the local extent of the lesion determines the characteristics and the severity of the aphasia [1]. In later publications, these ideas were further worked out, and his schemes also showed more connections between the various memory areas.3 Wernicke acknowledges that the motor and sensory centres may not be completely independent and that spoken language production relies to some extent on the auditory word form for the purpose of speech monitoring [18]. A careful reading of Wernicke’s original work thus reveals that he never proposed the serial and simple language model that later became one of the hallmarks of neurology.

Fig. 2.4
Wernicke’s model of how properties of words (ab) and the knowledge of objects [B, Begriff] are represented in the brain. B is the conceptual representation of an object. It is a construct of the association of acoustic (ac.), optical (opt.), tactical (tact.) and motor (mot.) images. The representation of the word (ab) that refers to an object consists of its auditory (a) and motor memory images (b) (Figure taken from de Bleser, 1996 [18])
There is a second important assumption that Wernicke makes in order to understand why a lesion of the auditory centre a will not induce lasting deficits in language comprehension [Begriff]. Wernicke states that area a and tract ab are very important in language comprehension, but only in childhood during language acquisition. In this phase, when language is learned, associative connections are formed between auditory and motor images.
Now the association of sound images with representations of movement essentially has its value in the fact that it makes it possible to learn language [1].
Once these associative connections have been established, the tract ab is predominantly used for repetition and is no longer critically involved in comprehension anymore.
Very soon after we have learned to speak a word, the intention of merely reproducing the sound disappears, making way for the intention of reproducing a specific meaning. The actual sensory images of an object [realen Sinnesbilder eines Gegenstandes], that is, are now able to innervate the representation of movement of a word [Bewegungsvorstellungen des Wortes] directly. (…) Later on, however, this pathway is no longer the one primarily used. Rather, the shorter pathways cb and db are chosen, and the mere existence of the pathway a1 b, without its being intentionally innervated, is sufficient to insure the choice of the correct representation of movement. [1]
So the areas that eventually sustain the information that is necessary to grasp the conceptual knowledge [Begriff] of any object are predominantly located outside the auditory language area a. This is stated quite boldly (and abruptly) in the monograph:
The concept [Begriff] is nothing more than the connection cd. [1]
Wernicke thus argues that once we have learned what a word means, the auditory or visual image of the word itself does not contribute much to the knowledge of the object (as it is not an innate property of it). In his own words:
The spoken and written name of an object is not a new attribute of the object. It is thus clearly different from the actual sensory memory images of the object. Only the latter make up the concept of the object. [1]
Using the example of the bell again:
The concept of a bell, for example, consists of memory images of visual, tactile, and auditory perceptions that are connected (associated) with each other. These memory images are essential attributes of the bell. The spoken word ‘bell’, however, has nothing in common with the acoustic impression that a bell makes on us, and there is likewise not the slightest similarity between the written word ‘bell’ and the image of a bell. (…) It is necessary to keep them apart. [1]
To Wernicke, loss of memory images that critically impair conceptual knowledge [Begriff] leads to asymbolia and not aphasia. He refers to Finkelnburg’s asymbolia, which he defines as ‘the loss of any memory images essential to the concept of an object’ [1]. Wernicke specifically adds that this can affect optical, tactile and also auditory images and also repeatedly stresses that language and intelligence are independent processes. He considers asymbolia a defect of intelligence and therefore not an aphasia:
Disturbances of the concepts of the things with which we deal in the process of thinking are always disturbances of intelligence; disturbances of language, on the contrary, cause difficulties only in the use of the conventional means [eingeführten Verkersmittel] of representation of the concepts. [1]
For Wernicke, ‘comprehension’ occurs at two different levels, so to speak. At the more superficial level, there is processing of auditory information and selection of auditory memory images. Deficits at this stage are considered a language comprehension disorder and will lead to a form of sensory aphasia. Then there is ‘comprehension’ at a more fundamental and conceptual level, where knowledge itself is stored. In modern terms, we would define the asymbolia of Wernicke and Finkelnburg as a form of agnosia: a not knowing or not recognizing of specific sensory stimuli. In later papers, Wernicke was more explicit on how these different concepts related. In fact, Wernicke was an expert on this topic, as he was the mentor of authors who wrote seminal papers on agnosia (see also Chap. 3). In a paper published in 1886, Wernicke wrote:
It may be helpful to bear in mind that more precisely two activities must be differentiated in language comprehension. In the first step, the concept of the word is activated, in the second one, the concept of the corresponding object. The process is similar in spontaneous speech, but in the reverse order, so that first the concept of the object arises and then that of the word. [18]
2.3.2.1 A Modern Definition of Wernicke’s Aphasia
In Mesulam’s Principles of Behavioral and Cognitive Neurology, Damasio describes the key features of a modern definition of Wernicke’s aphasia [19]. There is fluent and often unintelligible speech, and patients have difficulty with selection of the words (resulting in semantic paraphasias) or with the order of sounds (resulting in phonological paraphasias). In addition to that, there are important problems with auditory comprehension of sentences. Damasio describes that Wernicke’s area itself is not the centre where auditory comprehension takes place, in terms quite similar to Wernicke’s own formulations in his monograph:
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


