22 Microsurgical and Endoscopic Anatomy of the Parasellar Region
Carolina Martins, Alexandre Yasuda, Alvaro Campero, Luiz Felipe de Alencastro, Kohei Inoue, and Albert L. Rhoton, Jr.
 Introduction
Introduction
The parasellar area is part of the middle fossa, between the sellae and the temporal fossa. The parasellar area is considered to be the smallest area of the skull base with the highest concentration of important neural and vascular structures, as it houses the cavernous sinus.
The cavernous sinuses are bordered by the petrous apex and dorsum sellae posteriorly and by the superior orbital fissure anteriorly. They extend from the level of the foramen rotundum inferiorly up to the level of the clinoids. Each cavernous sinus has four walls. The roof faces the basal cisterns. The posterior wall faces the upper part of the posterior fossa. The medial wall, which separates the cavernous sinus from the contents of sella and sphenoid sinus, is formed by a thin dural layer, and this anatomical fact enables sellar tumors to extend toward the cavernous sinus. The lateral wall faces the medial temporal lobe. It has an inclination from medial to lateral, and is continuous with the floor of the temporal fossae.
Because of its acute-angled front and the shape of its back, the cavernous sinus has been compared with a boat.1 It can also be viewed as a tent, in which fixed structures are covered by a cloth to create a compartment. In the cavernous sinus, these fixed structures belong to the skull base, and the cloth above them is the dura.
Knowledge of this special architecture is paramount in performing surgery in the parasellar area. The need to better understand the cavernous sinus has been a relentless effort, which started through a series of important anatomical contributions,2–4 paving the way to the present understanding of the area.5–8
 Bone Structures Along the Parasellar Area
Bone Structures Along the Parasellar Area
The parasellar area is formed by a small contribution of the temporal bone and a major part of the sphenoid (Fig. 22.1). The temporal bone contributes to the parasellar area with its petrous apex, medial to the trigeminal impression. The petrous apex faces the lingula of the sphenoid bone and forms the posterior lip of the cranial opening of the carotid canal. In the articulated skull, both the lingula and the petrous apex are linked by the petrolingual ligament, which separates the petrous from the first vertical portion of the cavernous carotid. The sphenoid bone, the major bone structure responsible for supporting the cavernous sinuses, presents to the parasellar area the anterior clinoid process and the lateral part of the sphenoid body, along which the greater sphenoidal wing attaches.
The lesser sphenoid wings attach to each other along the sphenoid planum. Their posterior edges, the sphenoidal ridges, end medially as the anterior clinoid processes. Medial to the anterior clinoids are the intracranial openings of the optic canals, and, between them, the chiasmatic sulcus. The tuberculum sellae separates the chiasmatic sulcus and sphenoid planum from the sella turcica. On the most lateral part of this area the medial clinoid process may be present. In some instances, this process is linked to the anterior clinoid, forming the carotico-clinoidal foramen, through which the carotid artery passes. Across the sella, the tuberculum faces the dorsum sellae. On each side of dorsum, are the posterior clinoid processes.
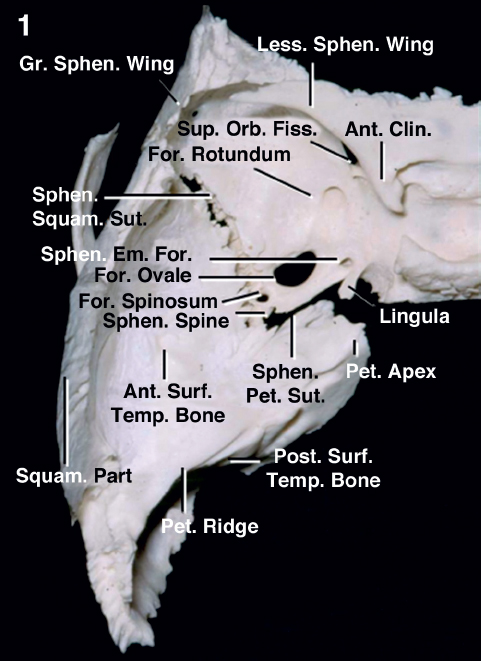
Fig. 22.1 Bone structures of the parasellar area. Ant.: anterior; Clin.: clinoid, clinoidal; Em.: emissary; Fiss.: fissure; For.: foramen; Gr.: greater; Less.: lesser; Orb.: orbital; Pet.: petrous, petrosal; Post.: posterior; Sphen.: sphenoidal; Squam.: squamosal; Sup.: superior; Sut.: suture; Temp.: temporal.
The lateral part of the body of the sphenoid forms the inferior part of the medial wall of the cavernous sinus, which extends from the petrous apex to the superior orbital fissure. The upper part of the medial wall, up to the clinoids, is directly related to the contents of the sella. The portion of the sphenoid body that is related to the medial wall presents the carotid sulcus. The carotid sulcus runs along the lateral surface of the body of the sphenoid from its posterior part, near the lingula, where this sulcus is deeper, toward the superior orbital fissure, where the carotid sulcus fades along the optic strut. The carotid sulcus is the impression left at the body of the sphenoid by the carotid artery (Fig. 22.2).
To understand the structure of the cavernous sinus is fundamental to understanding the anterior clinoid and its attachments. Each anterior clinoid is attached to the sphenoid by three points (Fig. 22.3). Laterally, the anterior clinoid is continuous with the sphenoid ridge. Medially, the anterior clinoid attaches to the sphenoid by its anterior and posterior roots. The anterior root passes medially over the optic canal and along the sphenoid planum. This bone often is defective and very thin, and the dura is the only element protecting the optic nerve in this area. The posterior root, also called the optic strut, is usually stout. It links the anterior clinoid to the sphenoid body, separating the optic canal from the superior orbital fissure. As the roof and floor of the optic canal are clinoidal attachments, the removal of the anterior clinoid decompresses the optic nerve.
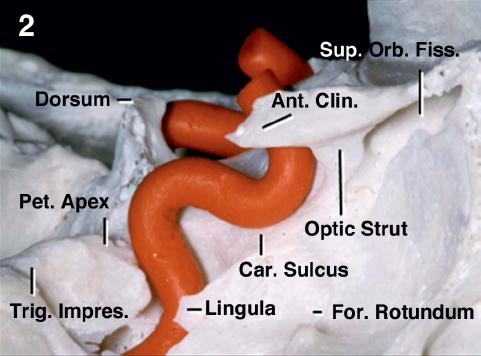
Fig. 22.2 Lateral view along the parasellar area. The internal carotid artery is shown in red. The lateral portion of the sphenoid body presents the carotid sulcus, the impression left at the body of the sphenoid by the carotid artery. Ant.: anterior; Car.: carotid; Clin.: clinoid; Fiss.: fissure; For.: foramen; Impres.: impression; Orb.: orbital; Pet.: petrous; Sup.: superior; Surf.: surface; Trig.: trigeminal.
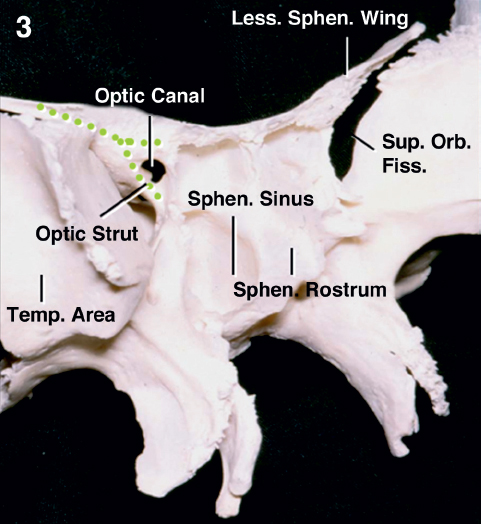
Fig. 22.3 Anterior oblique view of the sphenoid bone helps in understanding the anterior clinoid attachments. Fiss.: fissure; Less.: lesser; Orb.: orbital; Sphen.: sphenoidal; Sup.: superior; Temp.: temporal.
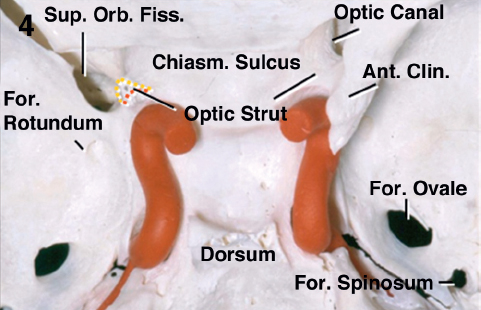
Fig. 22.4 Posterosuperior view into the parasellar area. The anterior clinoid process has been removed on the left, exposing the optic strut. The optic strut has two neural-facing surfaces, related to structures passing along the superior orbital fissure and optic canal (yellow dotted lines) and a vascular-facing surface, which relates to the carotid artery (red dotted line). Ant.: anterior; Chiasm.: chiasmatic; Clin.: clinoid; Fiss.: fissure; For.: foramen; Orb.: orbital; Sup.: superior.
The optic strut has three surfaces. The surface facing superiorly is the floor of the optic canal, the surface facing laterally forms, with the sphenoidal body, the medial border of the superior orbital fissure and is located at the anterior end of the cavernous sinus. The posterior-facing surface of the optic strut is concave and adapts to the anterior bend of the clinoidal portion of the carotid artery (Fig. 22.4). When removing the anterior clinoid—a common step in dealing with the cavernous sinus—the surgeon must recall that the optic strut has two neural-facing surfaces, related to the structures passing along the optic canal and superior orbital fissure, and a third, vascular-related surface, which faces the carotid.
Knowledge about the anterior clinoid is also important in understanding the roof of the cavernous sinus. The real roof of the sinus is located below the level of the anterior clinoid. The clinoid and its dural covering are extra protections for the anterior part of the roof, and can be compared to the attic of a house. At the level of the anterior clinoid, the carotid artery passes along the dural coverings of the parasellar area to reach the subarachnoid space. The part of the artery at the level of the anterior clinoid is not fully cavernous nor completely subarachnoidal, but is enclosed in this clinoidal intermediate space or attic and is named the clinoidal carotid.5
Mastering the anatomy of the anterior clinoid and clinoidal segment of the carotid is also paramount when dealing with the lateral wall of the sphenoid sinus, through an exocranial, endoscopic route.
On the exocranial side, the bony depression into the medial end of the optic strut is the opticocarotid recess (Fig. 22.5). The broad round prominence below the opticocarotid recess overlies the structures passing through the superior orbital fissure. Above the recess, on the superolateral part of the sinus wall, the optic nerve and ophthalmic artery are enclosed in the dura of the optic canal. The superior and inferior edges of the opticocarotid recess mark the position of the upper and lower carotid dural rings, and the arterial segment located between the two is the clinoidal segment (Fig. 22.6).
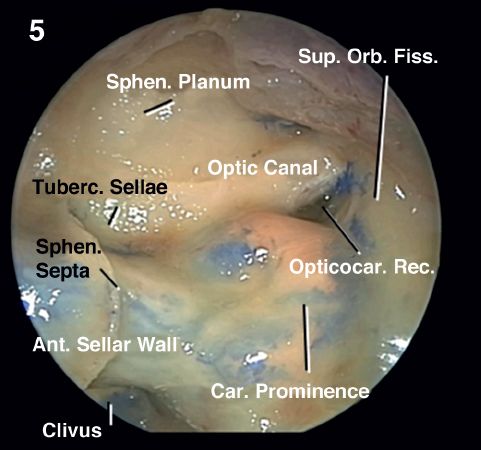
Fig. 22.5 Endoscopic dissection through the sphenoid sinus. The sphenoid planum and tuberculum sellae form the roof of the sphenoid sinus. The clivus, pneumatized up to the dorsum in this specimen, forms the posterior wall. The sella is located on the transition between the roof and posterior wall of the sphenoid sinus. The carotid sulcus produces a prominence within the sphenoid sinus, which is maximal in the most pronounced pneumatized sinuses. The carotid prominence can be divided into three segments: retrosellar, infrasellar, and presellar. Ant.: anterior; Car.: carotid; Fiss.: fissure; Opticocar.: opticocarotid; Orb.: orbital; Rec.: recess; Sphen.: sphenoidal; Sup.: superior; Tuberc.: tuberculum.
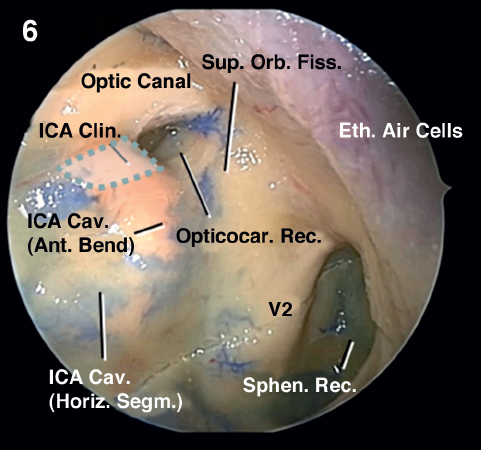
Fig. 22.6 Superolateral wall of the sphenoid sinus (left side); the clinoidal segment is highlighted by the dotted line. Ant.: anterior; Cav.: cavernous; Clin.: clinoid, clinoidal; Eth.: ethmoid, ethmoidal; Fiss.: fissure; Horiz.: horizontal; ICA: internal carotid artery; Opticocar.: opticocarotid; Orb.: orbital; Rec.: recess; Segm.: segment; Sphen.: sphenoidal; Sup.: superior; V2: second trigeminal nerve.
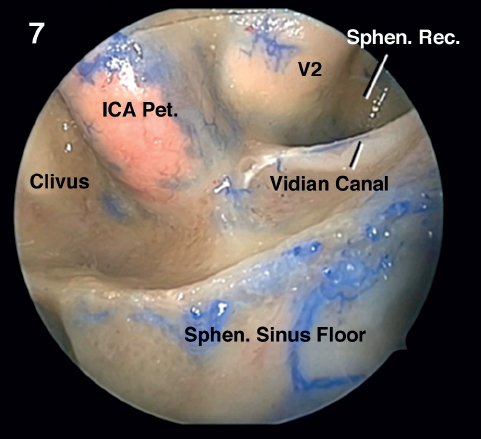
Fig. 22.7 Inferolateral wall and floor of the sphenoid sinus. As the cavernous sinus ends inferiorly at the level of the maxillary division (V2), the sphenoidal recess extends laterally below the sinus and lateral to the petrous part of the carotid artery. This segment of the carotid artery is signaled by the position of the vidian canal, which can be seen coursing along the floor of the sphenoid sinus. The vidian canal transmits the vidian nerve and the vidian artery. The vidian nerve is formed by the combination of the deep carotid nerve and the greater petrosal nerve and courses from the anterior wall of the foramen lacerum to the pterygopalatine ganglion into the pterygopalatine fossa. ICA: internal carotid artery; Pet.: petrous, petrosal; Rec.: recess; Sphen.: sphenoidal.
A segment of the maxillary division of the trigeminal nerve, just peripheral to the ganglion, protrudes into the lateral wall, below the sella. The average length of the maxillary division bulging into the sinus is 10.9 mm.3 The trigeminal ganglion and the first and third trigeminal divisions are usually separated from the sinus wall by the position of the carotid artery; however, when the sphenoid sinus is fully pneumatized into the greater sphenoid wing, creating the sphenoid sinus recess, the maxillary division becomes more clearly defined and the position of the superior orbital fissure and the mandibular division may be more clearly identified (Figs. 22.6 and 22.7).
 Cavernous Sinus Contents
Cavernous Sinus Contents
The dural envelope of the cavernous sinus is the site of a venous confluence that receives the terminal end of multiple veins draining the orbit, the sylvian fissure, and the middle and anterior fossae, and it has free communications with the basilar, superior and inferior petrosal and the intercavernous sinuses (Fig. 22.8). The three main venous spaces within the sinus are identified by their relation to the carotid artery; they are the medial, anteroinferior, and posterosuperior compartments.
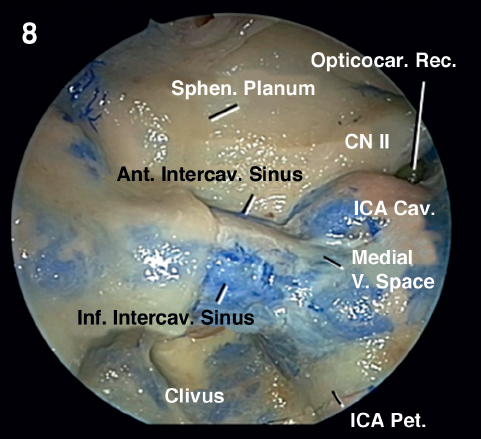
Fig. 22.8 The bone has been removed over the left half of the sellae and lateral wall of the sphenoid sinus. The retrosellar segment of the carotid prominence is seen on the posterolateral part of the sinuses in which the pneumatization extended laterally in the area of the dorsum. The retrosellar carotid prominence comprises the transition part between the distal petrous and the proximal cavernous carotid and is bound in place laterally by the petrolingual ligament. Several venous connections link the cavernous sinuses across midline, including the anterior and inferior intercavernous sinuses. These transsellar connections between the cavernous sinuses may exist at any point from the anterior to the posterior wall of the sella, including the diaphragma, or all connections between the two sides may be absent. The anterior intercavernous sinus, crossing the upper anterior margin of the sella, joins the cavernous sinus immediately behind the site at which the upper and lower rings fuse. The largest and most constant intercavernous connection is the basilar sinus, passing posterior to the dorsum and upper clivus and connecting the posterior aspect of both cavernous sinuses. The three main venous spaces within the sinus are identified by their relation to the carotid artery; they are the medial, anteroinferior, and posterosuperior compartments. Ant.: anterior; Cav.: cavernous; CN: cranial nerve; ICA: internal carotid artery; Inf.: inferior; Intercav.: intercavernous; Opticocar.: opticocarotid; Pet.: petrous; Rec.: recess; Sphen.: sphenoidal; V.: vein, venous.
Besides the medial venous plexus, the most medial structure inside the cavernous sinus is the carotid artery, coursing in intimate relationship with the abducens nerve (Figs. 22.8, 22.9, 22.10, 22.11, 22.12, and 22.13). The terminal part of the petrous carotid exits the carotid canal and passes under the trigeminal nerve and the petrolingual ligament, where it turns upward to enter the posterior part of the cavernous sinus. The artery becomes enclosed in the dural envelope of the cavernous sinus only when it exits the region of the foramen lacerum and turns upward, after traveling below the petrolingual ligament to reach the carotid sulcus on the lateral surface of the sphenoid body.
The third and fourth nerves enter the posterior part of the roof, in close relation with the meningohypophyseal branch, and reach the lateral wall of the cavernous sinus, to pass, with the first trigeminal division, along the superior orbital fissure. The abducens nerve can be well seen when the first trigeminal division is displaced laterally (Fig. 22.12). The abducens nerve passes through the lower margin of the posterior wall of cavernous sinus, under the petrosphenoid ligament (Gubler’s ligament). It courses inside the cavernous sinus and receives branches of the carotid nerve.
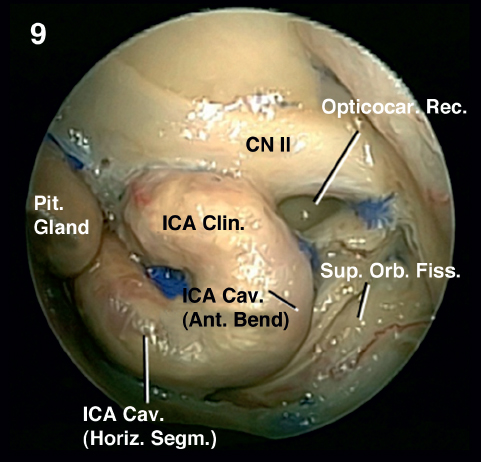
Fig. 22.9 The dura and venous structures have been removed, exposing the relationship of the carotid and pituitary gland. The infrasellar segment of the carotid prominence is located below the sellar floor and comprises the horizontal portion of the cavernous carotid. The presellar segment is located beside the anterior sinus wall and is the most frequently identified prominence related to the carotid inside the sphenoid sinus. It comprises the anterior carotid bend and the clinoidal segment of the carotid artery. The bone separating the artery and the sphenoid sinus is thinnest along the presellar part just below the tuberculum sellae. Ant.: anterior; Cav.: cavernous; Clin.: clinoid; CN: cranial nerve; Fiss.: fissure; Horiz.: horizontal; ICA: internal carotid artery; Opticocar.: opticocarotid; Orb.: orbital; Pit.: pituitary; Rec.: recess; Segm.: segment; Sup.: superior.
Related posts:
 External Versus Endoscopic Approaches for Skull Base Malignancies
External Versus Endoscopic Approaches for Skull Base Malignancies
 Anatomical Basis of Skull Base Surgery: Skull Osteology
Anatomical Basis of Skull Base Surgery: Skull Osteology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


