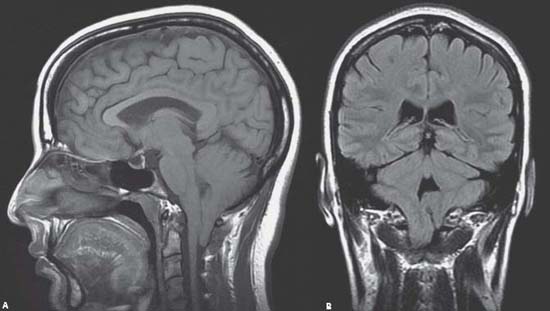
Case 100 Chiari I Malformation Fig. 100.1 (A) Sagittal and (B) coronal T2-weighted magnetic resonance images, demonstrating small posterior fossa, descended cerebellar tonsils down to the level of C1–C2 level posteriorly, and compression of the cranio–cervical junction and cervical spinal cord.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
100 Chiari I Malformation
Only gold members can continue reading. Log In or Register to continue


Full access? Get Clinical Tree


