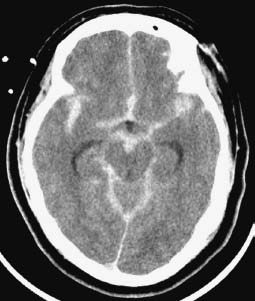
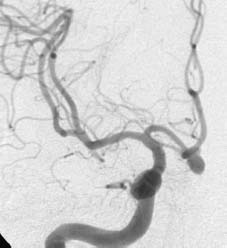
Case 30 Subarachnoid Hemorrhage and Vasospasm Fig. 30.1 Computed tomography of the head axial cut through basal cisterns. Fig. 30.2 Cerebral angiogram, anteroposterior view, right carotid injection. Fig. 30.3 Cerebral angiogram, antero-posterior view, right carotid injection, performed 6 days later, after a therapeutic intervention.

 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue




