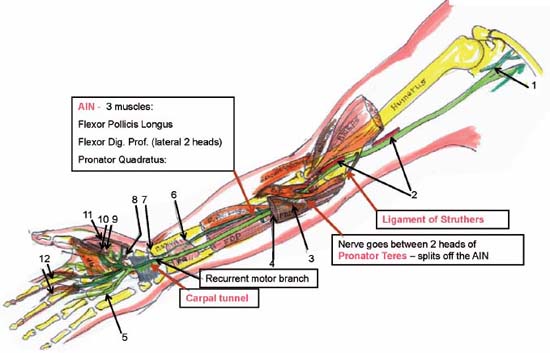
Case 101 Median Nerve Entrapment at the Wrist Fig. 101.1 Artist’s rendering of median nerve anatomical course and locations of entrapment. Sites of en trapment are highlighted in pink. AIN, anterior interosseous nerve; FDP or Flexor Dig. Prof., flexor digitorum profundus; PQ, pronator quadrates; AP, adductor pollicis; PT, pronator teres; F. Pol. Longus, flexor pollicis longus; FDS, flexor digitorum superficialis. (1) Lateral and medial cords join to form the median nerve. (2) Median nerve descends along the medial edge of the brachial artery. (3) Median nerve passes under the flexor digitorum superficialis (arcade forms the Sublimis Bridge). (4) Median nerve descends between flexor digitorum superficialis and profundus. (5) Sensory branches of the median nerve. (6) Anterior interosseous nerve (AIN) reaches deep to the pronator quadrates. (7) AIN gives off the wrist articular branches. (8) Recurrent motor branch variation. (9) Abductor pollicis. (10) Flexor pollicis. (11) Opponens pollicis. (12) Lumbricals I and II.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
101 Median Nerve Entrapment at the Wrist
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


