Case 106 Lower Extremity Peripheral Nerve Sheath Tumor
Robert L. Tiel
- A 15-year-old right-handed boy presented with a lump on the posterior lateral aspect of his right leg, just above the popliteal crease.
- Although the lump is usually painless, if knocked or manipulated he experiences a shooting sensation down his leg into the side and top of his foot.
- The frequent pains thus generated have forced him to abandon playing soccer.
- His neurologic examination is normal.
- When the lump is palpated it seems to have the dimensions of a large olive-sized (2 × 2 × 2-cm) mass. It moves from right to left, but not vertically. When lightly percussed, a sharp sensation is elicited, which goes into the dorsum of the right foot.
- Other physicians had previously seen the patient. After a magnetic resonance imaging (MRI) scan had been obtained (Fig. 106.1), they advised him to have the lump monitored, to limit his activities, and to “live with” the condition.
Fig. 106.1 T1-weighted contrast-enhanced magnetic resonance image of a schwannoma. Note widening of the nerve.
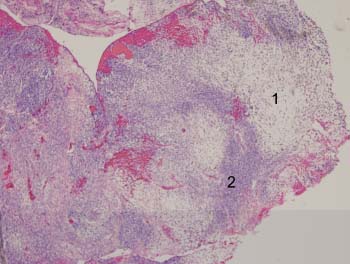
Fig. 106.2 Low magnification (40×) of tumor with two areas of interest (hematox ylin and eosin [H&E] stained).
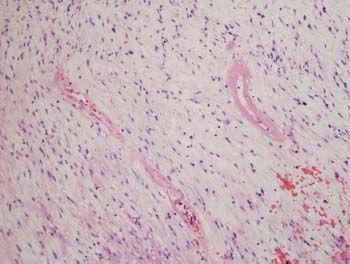
Fig. 106.3 High magnification (200×) of area 1 (H&E) stained).
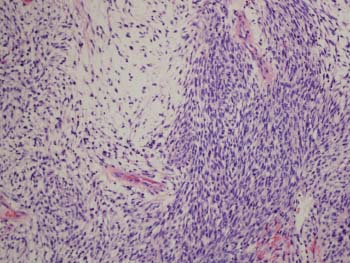
Fig. 106.4 High magnification (200×) of area 2 (H&E stained).
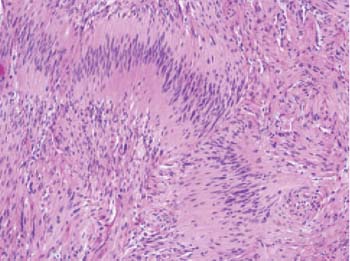
Fig. 106.5 High magnification (200×) of tumor pathology (H&E stained).
< div class='tao-gold-member'> Clinical Presentation
Clinical Presentation Questions
Questions
 Answers
Answers


