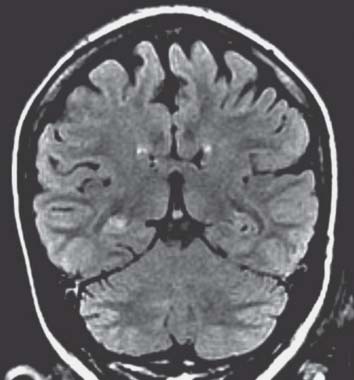
Section III Neurology Abdulrahman J. Sabbagh, Lahbib B. Soualmi, Fawziah A. Bamogaddam, Khurram A. Siddiqui, and Shobhit Sinha She had video electroencephalography (EEG) monitoring that showed ictal and interictal evidence of a right temporal focus. A magnetic resonance imaging (MRI) scan of the brain is performed (Fig. 108.1). Neuropsychological evaluation reveals normal intelligence, verbal and visuospatial memory. She was shown to be strongly left hemisphere dominant, and Wada test lateralized her verbal functions, memory, and speech to the left side. Fig. 108.1 Fluid-attenuated inversion-recovery coronal magnetic resonance image of the brain.
Case 108 Temporal Lobe Epilepsy
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
108 Temporal Lobe Epilepsy
Section III Neurology Fig. 108.1 Fluid-attenuated inversion-recovery coronal magnetic resonance image of the brain.
Case 108 Temporal Lobe Epilepsy
Clinical Presentation
Questions
Answers
< div class='tao-gold-member'>
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


