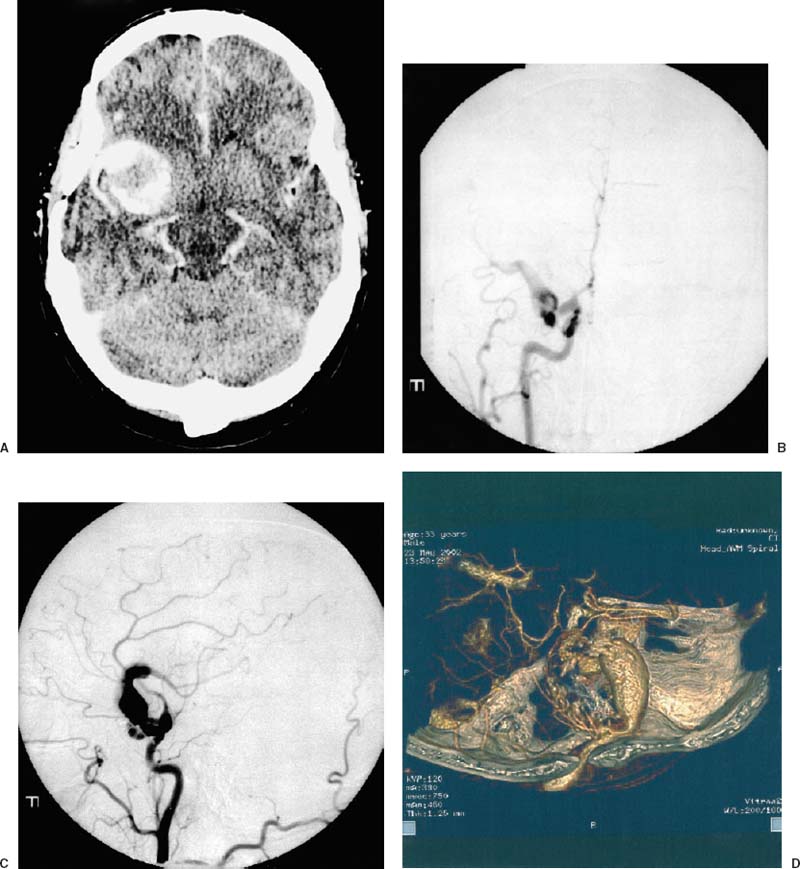
11 Diagnosis Giant fusiform aneurysm of middle cerebral artery Problems and Tactics A middle cerebral artery (MCA) aneurysm previously clipped after subarachnoid hemorrhage was found to have recurred with fusiform dilation of the M1 segment in a neurologically asymptomatic patient. We first treated the lesion surgically with flow reversal using extracranialintracranial (EC-IC) bypass from the external carotid to the M2 segment inferior division and clipping of the internal carotid distal to the ophthalmic segment. The patient presented after a syncopal episode with continued growth of the aneurysm. We elected to treat him endovascularly with trapping of the proximal aspect of the M1 aneurysm with endovascular coils after balloon test occlusion. On follow-up, the M1 segment has thrombosed without clinical sequelae. Keywords Fusiform aneurysm, EC-IC bypass, endovascular coiling, middle cerebral artery This 31-year-old male service technician was awoken from sleep with a severe headache in 1994. He was found to have a giant middle cerebral aneurysm and underwent clipping at an outside hospital, resulting in minor left monoparesis, which resolved soon after surgery. Several years later, head computed tomography (CT) was performed following a syncopal episode. This scan demonstrated a partially thrombosed, giant aneurysm of the middle cerebral artery (MCA). Neurological examination remained normal. Angiography showed a fusiform aneurysm beginning at the origin of the M1 segment and extending to the bifurcation, with some abnormal enlargement of the distal internal carotid artery (ICA) at the level of the anterior choroidal artery and the proximal anterior cerebral artery. No posterior communicating artery was present (Fig. 11–1). We proceeded with a bypass procedure to reverse the direction of flow in the aneurysmal M1 segment by creating an external carotid to MCA bifurcation graft with surgical clip ligation of the internal carotid artery just beyond the origin of the ophthalmic artery (Fig. 11–2). The patient did well until 2 years later, when he suffered a second syncopal event. A repeat head CT showed further enlargement of the partially thrombosed aneurysm. He remained asymptomatic. At that point, we proceeded with endovascular trapping of the aneurysm by temporarily occluding the M1 segment between the site of the graft anastomosis and the aneurysm, allowing the A1 segment and distal internal carotid artery to fill retrograde from the anterior communicating artery and preserving the anterior thalamostriate arteries. The proximal M1 was then endovascularly occluded with detachable coils near its origin off the ICA (Fig. 11–3). Follow-up angiography at 8 months demonstrated interval thrombosis of the M1 segment (Fig. 11–4). A CT scan showed no further growth. He has remained asymptomatic. FIGURE 11–1 Preoperative head computed tomographic scan and angiogram showing (A) a large, right-sided aneurysm with calcium and (B–D) the anterior, posterior, and lateral view of the fusiform, partially thrombosed middle carotid artery aneurysm.
Giant Fusiform Aneurysm of the Middle Cerebral Artery
Clinical Presentation
Stage 1: Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


