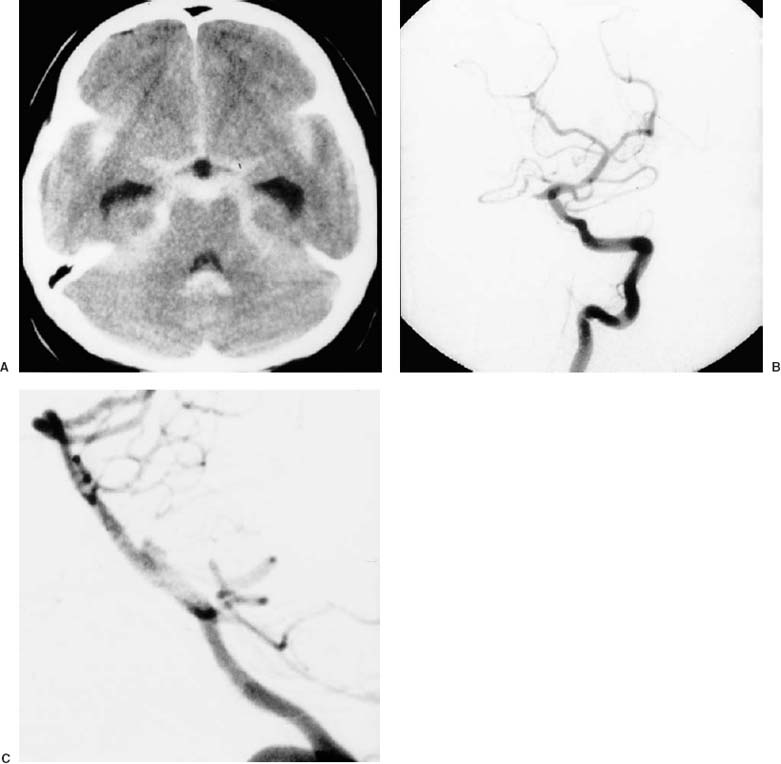
17 Diagnosis Basilar trunk aneurysm Problems and Tactics A basilar trunk aneurysm at the origin of the anterior inferior cerebellar artery was identified as the cause of subarachnoid hemorrhage. The aneurysm was safely secured using the retrolabyrinthine presigmoid approach and a satisfactory outcome was obtained. Keywords Basilar trunk aneurysm, retrolabyrinthine approach This 42-year-old woman complained of a suddenly developed headache, accompanied by nausea and vomiting. She had no previous history of illness. Computed tomography (CT) showed subarachnoid hemorrhage involving the basal cistern and the sylvian fissures bilaterally (Fig. 17–1). Intraventricular hemorrhage was also noted in the fourth ventricle. Vertebral angiograms revealed an aneurysm in the midbasilar trunk and at the origin of the anterior inferior cerebellar artery (AICA) (Fig. 17–1). The aneurysm projected toward the right side and in a posterior direction. A lumbar drainage catheter was inserted after inducing general anesthesia. The patient was placed in the supine oblique position. A curved incision was made behind the ear, from the posterior temporal area to the tip of the mastoid process. A craniotomy, including the right temporal and suboccipital regions, was performed after making four burrholes, as described previously.1 The lateral and sigmoid sinuses were exposed. An L-shaped mastoidectomy was performed using a high-speed drill with continuous irrigation. The anterior border of the mastoidectomy was a curved line from the external auditory meatus to the mastoid tip, and the superior border was perpendicular to the anterior border, starting from the zygomatic root.2 Exposed air cells were occluded with bone wax to prevent cerebrospinal fluid leakage. Bone bleeding was also controlled with bone wax. The sigmoid and distal lateral sinuses were uncovered, and Citelli’s angle, which identifies the position of the superior petrosal sinus (SPS), was exposed. Bone was removed over these sinuses using gentle strokes, leaving a thin bony shell over the sinuses that prevented sinus laceration. A mastoid emissary vein was controlled with a bipolar coagulator near its entrance to the sigmoid sinus. Posterior petrous bone was removed while preserving the labyrinthine structure and the fallopian canal. Presigmoid dura in Trautmann’s triangle was exposed between the bony labyrinth and the sigmoid sinus (Fig. 17–2). A linear dural incision was made 5 mm anterior to the sigmoid sinus, extending up to the SPS (Fig. 17–2). A linear dural incision was also made in the temporal region, extending down to the SPS. The SPS was divided after hemoclip placement. With gentle retraction of the temporal lobe and cerebellar hemisphere the tentorium was exposed and incised 10 mm behind the SPS along the petrous ridge and up to the incisura. To avoid damage to the trochlear nerve the tentorial incision was made posterior to the dural entry of this nerve. FIGURE 17–1 Preoperative computed tomography and angiograms show (A) a dense subarachnoid hemorrhage, and (B, C) an aneurysm in the midbasilar trunk, projecting toward the right side and in the posterior direction. The basilar trunk was visualized between the seventh and eighth cranial nerve (CN) complex and the lower CNs after retraction of the lateral pons. The abducens nerve was encountered, running obliquely in a rostral direction below the seventh and eighth CN complex. After gentle dissection around the distal basilar trunk, a temporary clip was applied (Fig. 17–2
Basilar Trunk Aneurysm—Retrolabyrinthine Approach
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


