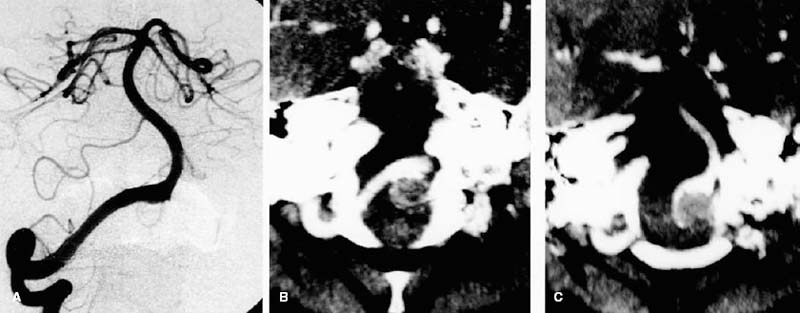
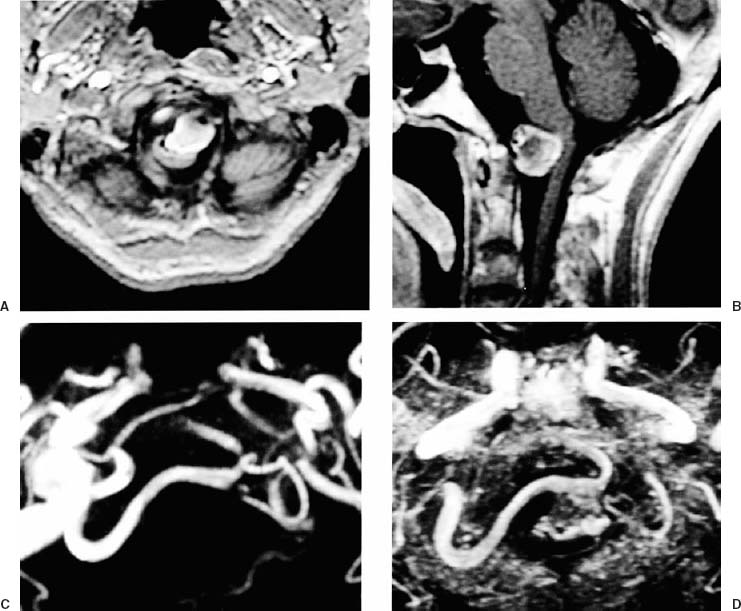
21 Diagnosis Large thrombosed vertebral artery aneurysm Problems and Tactics A large thrombosed aneurysm of the right vertebral artery was found in a 59-year-old man. The aneurysm’s neck crossed the midline and the dome was located on the left side. The left vertebral artery was hypoplastic. Because the common approach from the ipsilateral right side seemed extremely difficult, we attempted a direct clipping of the aneurysm via a left transcondylar approach with temporary intraoperative balloon occlusion of the right vertebral artery. Keywords Vertebral artery aneurysm, large thrombosed aneurysm, contralateral approach, temporary balloon occlusion, transcondylar approach This 59-year-old man had complained of persistent headache and nuchal pain for 6 months. Magnetic resonance imaging revealed an almost completely thrombosed aneurysm 24 mm in diameter on the left side in front of the medulla (Fig. 21–1). The right vertebral angiogram showed focal dilatation of the right vertebral artery with a retention of contrast medium at the site of the aneurysm (Fig. 21–2). The aneurysmal neck was beyond the midline to the left. The left vertebral artery was hypoplastic. The patient’s neurological status and somatosensory evoked potentials were stable during 20 minutes of test balloon occlusion of the right vertebral artery (V2 portion). After anesthesia was induced, an angiography catheter was introduced into the right vertebral artery (V2 segment) through a femoral sheath. A silicone balloon catheter was advanced through the angiography catheter and tentatively inflated to determine the volume needed to occlude the parent artery under fluoroscopic control. The systemic heparinization was achieved with intravenous heparin, and the catheter was flushed continuously with heparinized saline. The patient was then placed in the right modified semiprone park-bench position; his head was kept at maximal flexion, slightly face down and vertex to the floor. His temperature was maintained under mild hypothermia at 34 °C and somatosensory evoked potentials were monitored during surgery. The suboccipital bone and C1 lamina were completely exposed through a hockeystick skin incision. The emissary vein in the posterior condylar fossa was cut and the condylar fossa was dissected. A left lateral suboccipital craniotomy was carried to the midline and laterally to the sigmoid sinus. A C1 hemilaminectomy was performed across the midline. The foramen magnum was opened as wide as possible across the midline and laterally to the occipital condyle. From this point, the procedure was continued under the microscope. The dura mater over the left cerebellar hemisphere and the vertebral artery were retracted with spatulas, exposing the occipital condyle, condylar fossa, and jugular tubercle. With a high-speed drill, the posteromedial part of the occipital condyle, a part of the lateral mass of C1, and the jugular tubercle were drilled extradurally and removed. After the dura was opened, the aneurysmal dome compressing the medulla was seen under direct vision. The left vertebral artery, the left posterior inferior cerebellar artery, and the ninth, tenth, and eleventh nerves over the aneurysmal dome were observed after extensive arachnoid dissection (Fig. 21–3A). The right vertebral artery distal to the aneurysm was found, but the proximal portion of the right vertebral artery was hidden behind the large, thrombosed aneurysmal dome. FIGURE 21–1 (A, B) T1-weighted magnetic resonance image showing a large thrombosed aneurysm compressing the medulla posteriorly at the foramen magnum. (C, D) Magnetic resonance angiography showed the tortuous dominant right vertebral artery. The aneurysm was thrombosed and the aneurysmal neck crossed the midline to the left. FIGURE 21–2 (A) The right vertebral artery angiogram (anteroposterior view) showed the focal dilatation across the mid-line at the site of the aneurysm. There was no right posterior inferior cerebellar artery. (B, C) The postcontrast computed tomographic scan in the coronal plane clearly demonstrates the relationship between the right vertebral artery and the thrombosed aneurysm.
Contralateral Approach for a Large Thrombosed Aneurysm of the Vertebral Artery
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 26 A Large Cerebellopontine Angle Arteriovenous Malformation
26 A Large Cerebellopontine Angle Arteriovenous Malformation
 8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


