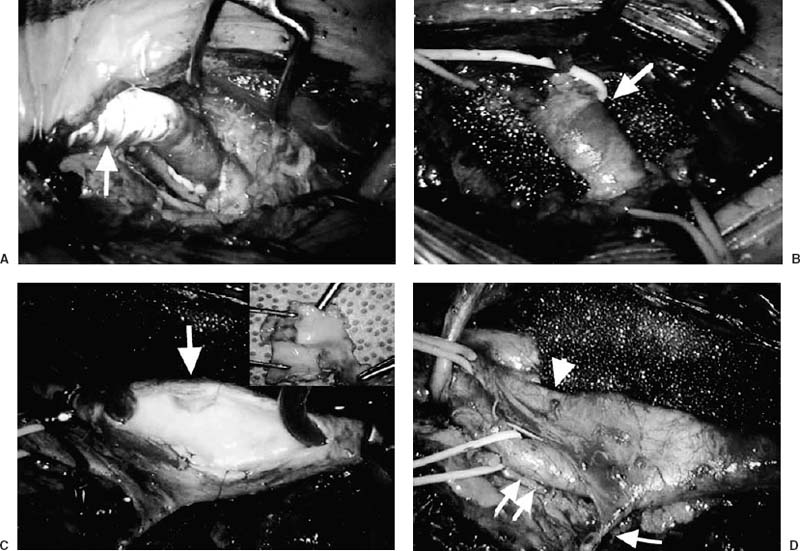
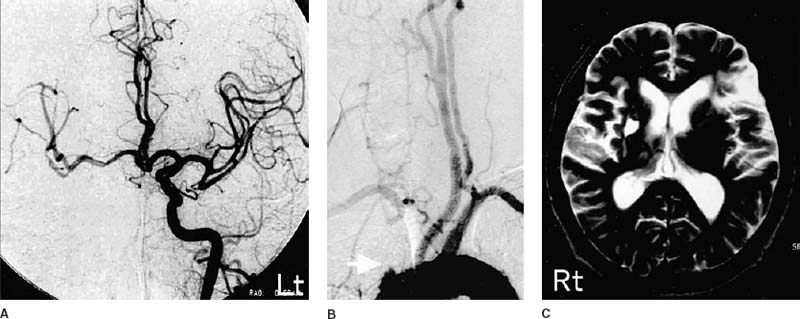
24 Diagnosis Right carotid endarterectomy and axilloaxillary bypass Problems and Tactics A patient suffering from transient left hemiparesis had innominate artery occlusion with right carotid stenosis. T2-weighted images demonstrated high-intensity lesions in the left frontoparietal region and in the right deep cerebrum. Cerebral blood flow (CBF) studies revealed an evident low perfusion area in the right cerebral hemisphere. To improve the compromised cerebral hemodynamics, axilloaxillary bypass and right carotid endarterectomy were performed in two stages. Keywords Compromised cerebral hemodynamics, carotid stenosis, innominate arterial occlusion, carotid endarterectomy, axilloaxillary bypass This 69-year-old man had suffered from left hemiparesis. His right arm blood pressure was ~30 mmHg lower than that of the left side. Magnetic resonance imaging (MRI) revealed high-intensity lesions in the left frontoparietal region and in the right deep cerebrum (Fig. 24–1C) on T2-weighted images. Aortogram showed innominate artery occlusion, left carotid stenosis (40%) at the cavernous portion, right cervical carotid stenosis (60%), and left vertebral artery stenosis at its origin from the subclavian artery (Fig. 24–1B). The left carotid angiogram demonstrated an excellent anterior cross-circulation well visualizing the right middle and anterior cerebral arterial territory (Fig. 24–1A). CBF studies with the cold xenon–computed tomographic (Xe-CT) method revealed an evident decrease in blood flow in the right cerebral hemisphere with poor Diamox response. Two-staged reconstructive surgery consisting of axilloaxillary bypass and right carotid endarterectomy was planned to improve right carotid blood flow. In the first operation (axilloaxillary bypass), the patient was placed in the supine position under general anesthesia. Both arms were abducted 45 degrees in the horizontal plane. A bilateral infraclavicular incision (6 cm in length) was made to access the first portion of the axillary artery. The pectoralis major muscle was separated and the underlying pectoralis minor muscle was retracted laterally. Then the right and left axillary arteries were exposed (Fig. 24–2B). Heparin (3000 U) was intravenously injected, and activating coagulation time (ACT) was kept >200 seconds. First, the left axillary artery was occluded with a bulldog clamp at the proximal site and with a Sugita’s clip at the distal site. Axillary arteriotomy was made at the anterosuperior wall with a vascular punch (5 mm ID). A ring-supported, expanded polytetrafluoroethylene (ePTFE) graft with 5 mm ID (Gore-Tex vascular graft) was tunneled subcutaneously, passing anterior to the sternum. An end-to-side anastomosis between the graft and axillary artery was performed by running 6–0 Prolene sutures (Fig. 24–2A). The same preparation was done on the right side after adjusting the length of the graft. Leakage of the blood from the anastomosed site was observed just after declamping, which was easily controlled by application of fibrin glue to the site of the sutures. The patency of the bypass was excellent, with good pulsation of the involved axillary artery. FIGURE 24–1 (C) T2-weighted image shows high intensity spots at the right basal ganglia and high intensity area in the left frontoparietal region. (B) Panaortogram reveals innominate artery occlusion (arrow). (A) Left carotid angiogram demonstrates excellent anterior collateral blood flow. Rt, right; Lt, left. FIGURE 24–2 (B,A) Operative field shows the right axillary artery (arrow) and axilloaxillary bypass with expanded polytetrafluoroethylene (arrow). (D) The superior thyroid artery (single arrow), external carotid artery (double arrow), and internal carotid artery (arrowhead) are exposed. (Lower right) A shunt tube is indwelled and a stenotic lesion (arrow) is exposed. (C) An extirpated lesion shows intraplaque hemorrhage and calcification. The second operation was a carotid endarterectomy (CEA). The patient was placed in the supine position under general anesthesia. His head was moderately extended by fixing the jaw, and rotated to the left side ~20 degrees. Sensory evoked potentials (SEP) and blood flow with an electromagnetic flow meter (EMFM) were monitored during surgery. A curvilinear skin incision was made along the leading border of the right sternocleidomastoid muscle (SCM) toward the medial side of the clavicle. The platysma was cut, and connective tissues were dissected to open the carotid sheath. The common carotid artery (CCA) and external carotid artery (ECA) were then exposed, avoiding injuries to the hypoglossal, superior laryngeal, and vagus nerves. Because the internal carotid artery (ICA) was unusually located at the posteromedial site of the ECA, it was difficult to expose the ICA by the convenient procedure. The superior thyroid artery was therefore cut to pull the ECA laterally, and the involved ICA was exposed on the medial side of the ECA (Fig. 24–2D
A Case of Right Carotid Endarterectomy and Axilloaxillary Bypass for Symptomatic Carotid Stenosis with Innominate Artery Occlusion
Clinical Presentation
Surgical Techniques
Related posts:
 33 Removal of Vestibular Schwannoma in the Internal Auditory Canal with the Aid of Neuroendoscopy
33 Removal of Vestibular Schwannoma in the Internal Auditory Canal with the Aid of Neuroendoscopy
 26 A Large Cerebellopontine Angle Arteriovenous Malformation
26 A Large Cerebellopontine Angle Arteriovenous Malformation
 8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


