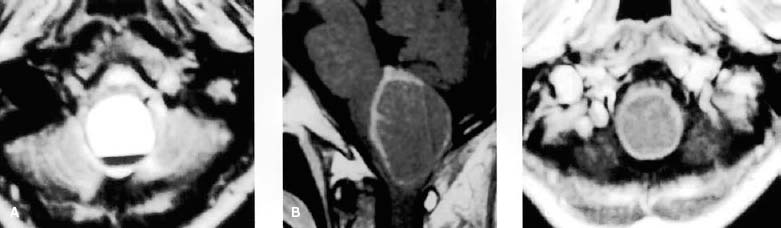
30 Diagnosis Ependymoma Problems and Tactics A large mass was found at the dorsal portion of the medulla oblongata in a previously healthy woman. Although high surgical risk was recognized, total removal of the tumor was performed for decompression of the medulla oblongata. Keywords Ependymoma, medulla oblongata, neuronavigation, intraoperative monitoring A previously healthy 58-year-old woman was admitted to the emergency room because of suffocation after accidental aspiration of water into the trachea. Physical examination showed difficulty in breathing and low grade fever, and chest radiograph revealed clouding of the lungs bilaterally. Neurological examination showed absence of gag reflex, diminished movement of the retropharyngeal wall, and diminished sensation (both superficial and deep sensation) in the four extremities. Computed tomography (CT) on admission showed a large, round, low-density mass at the Medulla oblongata. Plain magnetic resonace imaging (MRI) revealed niveau formation in the mass. Subsequent enhanced MRI revealed a ring enhancement (Fig. 30–1). The patient was placed in a prone position with her head moderately flexed. A linear skin incision was performed on the midline from the inion down to the C2, followed by osteoplastic craniotomy with partial removal of the C1 posterior arch. After durotomy in a Y-shaped fashion, the markedly enlarged medulla oblongata was exposed between the cerebellar tonsils beneath the arachnoid membrane. After dissection of the arachnoid membrane, aspiration of 20 mL of an old hematoma in the tumor was performed. The posterior median sulcus was carefully dissected, and then the relatively demarcated grayish tumor was observed. Several pieces of the tumor were removed for pathological diagnosis, and it was identified as metastatic carcinoma. To avoid deterioration of neurological function by performing total removal, subtotal removal of the tumor was performed. Neuronavigation and intraoperative electrical monitoring were used throughout the operative procedure. A second operation was planned because the diagnosis was corrected from metastatic carcinoma to atypical ependymoma by the permanent specimen (Fig. 30–2A,B). Using the previous wound, the residual tumor was exposed and was carefully removed from the surrounding medulla oblongata. The cleavage was relatively clear; however, adhesion was occasionally observed. While monitoring the tenth and twelfth cranial nerve function, total removal of the tumor was completed (Fig. 30–3). FIGURE 30–1 (A) T2-weighted magnetic resonance imaging (MRI) revealed niveau formation in a large mass suggestive of intratumoral hemorrage at the dorsal portion of the medulla oblongata. (B,C) Enhanced MRI revealed ring enhancement. Immediately after surgery, the patient had difficulty in swallowing and drinking despite good MRI results; however, no additional neurological deficits appeared. With daily rehabilitation of her retropharyngeal function, the patient became able to drink and eat 3 months postoperatively. She was discharged with reasonable recovery of sensation in all four extremities and restored swallowing function.
A Large Ependymoma with Intratumoral Hemorrhage in the Medulla Oblongata
Clinical Presentation
Surgical Technique
First Operation
Second Operation
Outcome
Key Points
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


