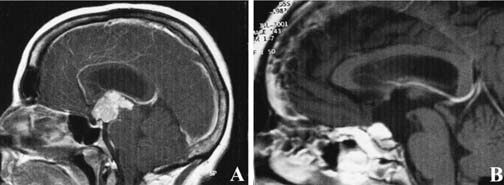
37 Diagnosis Suprasellar craniopharyngioma Problems and Tactics A large suprasellar craniopharyngioma was found during a workup for hypopituitarism and headache in an otherwise healthy young man. Although the lesion was largely suprasellar with extension into the anterior cranial fossa, a transsphenoidal approach was chosen with the aim of preserving visual function and avoiding more invasive transcranial techniques. Keywords Extended transsphenoidal approach, craniopharyngioma, suprasellar tumors A 32-year-old man presented with a 1-year history of impotence and loss of libido. General malaise, weight gain, and occasional moderate to severe headache were also present. The initial workup revealed the patient to have a low serum testosterone level of 30. Follicle stimulating hormone (FSH) and luteinizing hormone (LH) levels were also low at 0.6 and 1.3, respectively. The remainder of hormone levels were within normal limits. The physical exam was notable for mild breast enlargement and testicular atrophy. Visual fields were full to confrontation and on formal testing. Magnetic resonance imaging (MRI) scan revealed a very large multicystic lesion extending into the suprasellar space up to the floor of the third ventricle (Fig. 37–1). Imaging characteristics were consistent with craniopharyngioma. There was no associated hydrocephalus and the pituitary gland appeared normal but inferiorly displaced. The evening prior to surgery, the patient underwent a computed tomographic (CT) scan with fiducial markers for neuronavigation. After the induction of general anesthesia, a lumbar drain was placed. The patient was placed in the semirecumbent position with his head in a horseshoe headrest. The head was placed in a slight amount of extension. A sublabial approach to the sella was used in this case. First, endonasal submucosal dissection was performed through a standard hemitransfixation incision using loupe magnification. Anterior and posterior tunnels were developed within the nose to the anterior wall of the sphenoid sinus. A sublabial incision was then made and the inferior submucosal tunnels developed. At this point, the tunnels developed through the two incisions were connected, and a Hardy retractor was inserted to provide good exposure of the anterior wall of the sphenoid sinus. FIGURE 37–1 (A) Pre- and (B) postoperative images of a large suprasellar craniopharyngioma. A wide anterior sphenoidotomy was preformed in the standard manner to allow a full view of the stella, carotid, and optic protuberances. Using a small osteotome, the sellar floor was fractured, with care taken to avoid early dural compromise. The stella was widely opened using Kerrison rongeurs to expose the limits of the cavernous sinus laterally. At this point, using a high speed drill and angled bone punches, further bony removal proceeded along the planum sphenoidale and anterior cranial fossa floor. Frameless stereotaxy was used to guide the extent of bony removal. A large, superior, intercavernous sinus was carefully secured with vascular clips and cauterized with bipolar electrocautery before division.
A Case of Midline Suprasellar Tumor Removed by an Extended Transsphenoidal Skull Base Technique
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


