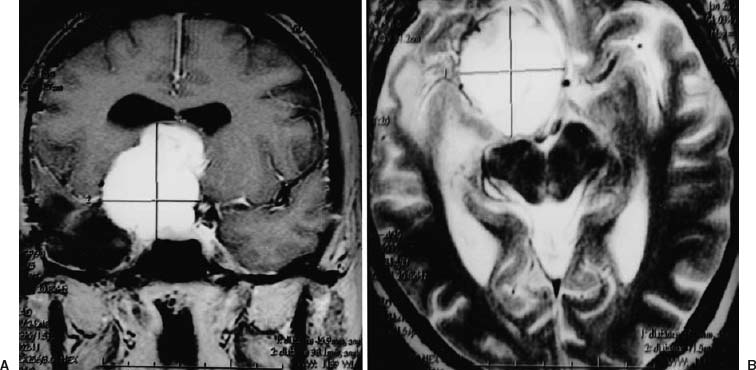
44 Diagnosis Giant right anterior clinoid meningioma Problems and Tactics A giant right anterior clinoid meningioma with lateroand suprasellar extension was found in a middle-aged woman. She was referred to an emergency service with an intracranial hypertension syndrome due to hydrocephalus secondary to obstruction of both the foramen of Monro and the third ventricle. The meningioma invaded the right carotid artery from the clinoid portion up to the bifurcation. A surgical cranial decompression was performed on emergency. Later the patient was referred to us for attempts at total removal of the tumor. The strategy consisted of performing a right extra–intracranial (EC–TC) bypass using a vein autograft for arterial revascularization of the carotid territory, followed by a complete gross tumor resection. The patient was then shunted for a normal pressure hydrocephalus that had persisted long term. Keywords Skull base meningioma, extra–intracranial (EC–IC) arterial bypass, interposed venous grafts, orbitozygomatic osteotomy This 44-year-old woman, a psychiatrist, was referred to an emergency service for disabling headaches and drowsiness in relation with a severe intracranial hypertension syndrome. Right-eye blindness with optic atrophy was found at ophthalmologic examination. Imaging demonstrated a right voluminous anterior clinoid meningioma with middle fossa and suprasellar extension compressing the third ventricle and foramen of Monro. Because of the severity of the clinical status, she had emergency decompressive partial resection of the tumor through a right frontotemporal craniotomy (Fig. 44–1). A few months later she was referred to our team for completing the surgery; namely, attempting total removal. Magnetic resonance imaging (MRI) showed the remaining portion of the tumor, developed from the anterior clinoid upward to the suprasellar region (Fig. 44–1). On right selective angiography, the C2 and C1 carotid artery, as well as the M1 segment of the middle cerebral artery, were found occluded by tumor invasion (Fig. 44–2). There was no cross-circulation from the left carotid artery; in fact, the right carotid bifurcation was occluded. Right hemisphere circulation was through a multitude of tiny meningeal–cortical anastomoses and cortical suppleances from anterior cerebral and posterior cerebral territories. In a first staged operation a right extracranial–intracranial (EC–IC) arterial bypass using internal saphenous venous autograft was performed between the lingual artery at the neck and the distal branch of the middle cerebral artery (namely, the angular artery). The decision to use a venous autograft was made because the superficial temporal artery had been destroyed at the first emergency surgery. The lingual artery was preferred because of its easy access at the neck and its appropriate caliber. An end-to-end anastomosis was completed with a dozen single stitches, using 8–0 nylon thread, between the lingual artery and the distal stump of the graft (taking into account the orientation of the valvulas). A subcutaneous tunnel was then created in the retroauricular region from the cervical incision to the cranial incision to pass the venous saphenous graft through, taking care to avoid twisting or kinking. FIGURE 44–1 (A) Coronal T1 magnetic resonance imaging (MRI) with gadolinium contrast and (B) axial T2 MRI showing a 5-cm right giant clinoid meningioma with suprasellar extension (and hydrocephalus). Notice displacement of the anterior and middle cerebral artery, located in a groove on the tumor capsule. Also note the temporal cavity corresponding to the previous surgical operation.
Giant Skull Base Meningioma Invading Carotid Artery
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


