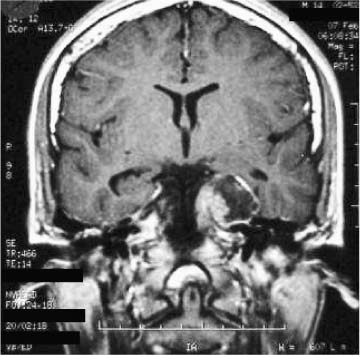
53 Diagnosis Dermoid cyst in the cavernous sinus Problems and Tactics Because of the complex anatomy of the cavernous sinus, few neurosurgeons have dared to approach the lesions of this region surgically. As a matter of fact, some tumors histologically benign have been allowed to become a malignant problem for the patient.1 The understanding of the bony and neurovascular contents of the “anatomical jewel box”2 permitted the development of modern skull base techniques, modifying the surgical morbidity and mortality as well as the natural history of some pathologies. Keywords Cavernous sinus, “peeling” of the middle fossa, dermoid cyst, surgical approach A 14-year-old boy was hospitalized in June 2002 with a 1-year history of progressive left hemicranial headache, some episodes of nausea, light-headedness, and seizures. Neurological examination showed trochlear paresis; V1, V2 hypoesthesia; and corneal reflex abolition on the left side. Computed tomographic (CT) scan demonstrated a well-demarcated lesion in the left cavernous sinus topography, with nonhomogeneous low intensity with a high intensity margin on T1-weighted magnetic resonance imaging (MRI) and high intensity with a low intensity margin on T2-weighted MRI. This lesion showed no enhancement by contrast media on either CT or MRI (Fig. 53–1). The patient was placed in the dorsal position. Through a left pretemporal orbitozygomatic craniotomy, the lateralmost aspect of the superior orbital fissure was exposed. The roof and lateral wall of the orbit were removed as far as the second division of the fifth nerve was visualized exiting the foramen rotundum. After the orbitomeningeal artery, a branch of the middle meningeal artery that goes into the orbit, was coagulated and cut, the dural tent over the superior orbital fissure was incised and gently peeled from the anterior portion of the lateral wall of the cavernous sinus. This maneuver exposed the oculomotor, trochlear, and first division of the trigeminal nerve. As the dissection proceeded in a posterior direction, the dura was peeled from the temporal bone to reach the foramen spinosum and expose the middle meningeal artery, which was coagulated and cut. The outer layer of dura was then peeled further from the cavernous sinus, exposing the second and third divisions of the fifth nerve and the gasserian ganglion. The course of the greater superficial petrosal nerve along the petrosphenoidal fissure could be well appreciated medial to the middle meningeal artery and posterior to V3. The intrapetrous carotid artery can be exposed in the petrous bone coursing parallel and inferior to the greater superficial petrosal nerve. At times, the intrapetrous carotid lacks any bony covering at this location. FIGURE 53–1 Preoperative T1 magnetic resonance image.
Approach to Lesions in and around the Cavernous Sinus: A Formidable Challenge
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


