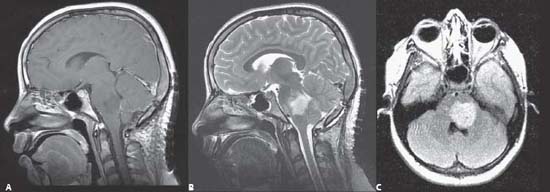
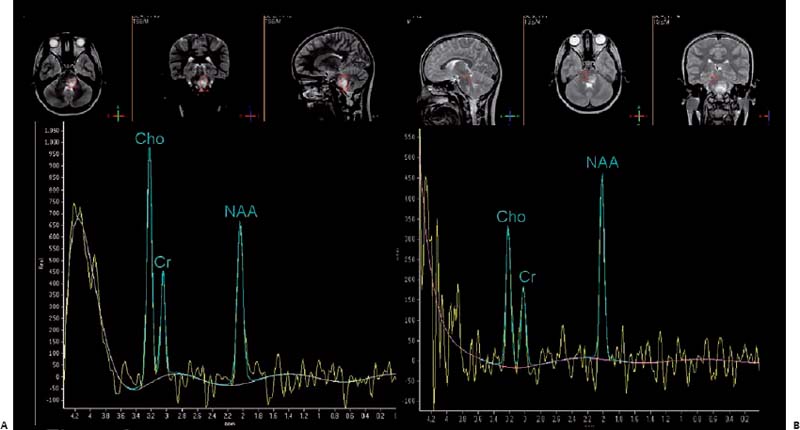
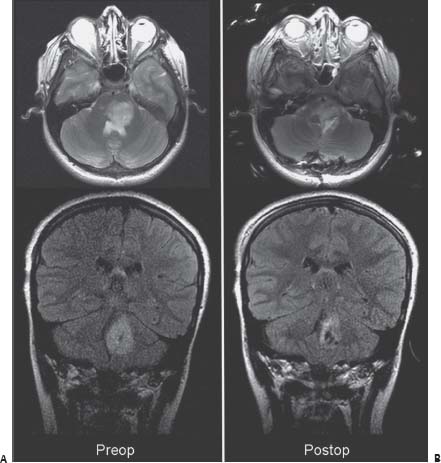
Case 58 Brainstem Glioma 1: Pons Fig. 58.1 (A) Brain sagittal T1-weighted magnetic resonance image (MRI) with gadolinium, (B) sagittal T2-weighted MRI and (C) axial fluid-attenuated inversion-recovery (FLAIR) image through the pons. Fig. 58.2 Magnetic resonance spectroscopy showing voxel configuration taken within the tumor (A) and within normal pons (B). Fig. 58.3 Comparison bet ween (A) preoperative and (B) postoperative magnetic resonance images showing axial T2-weighted and coronal fluid-attenuated inversion-recovery images taken at the level of the pontine tumor.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
58 Brainstem Glioma 1: Pons
Only gold members can continue reading. Log In or Register to continue


Full access? Get Clinical Tree


