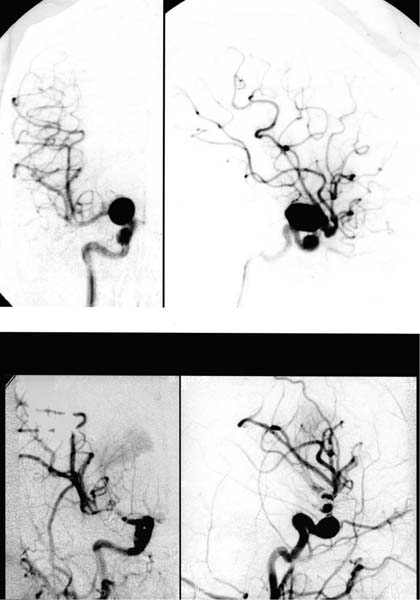
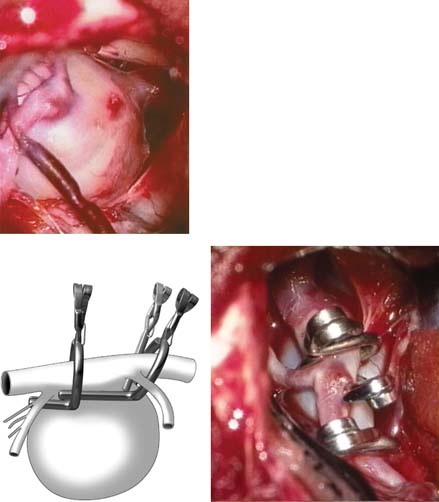
7 Diagnosis ICA giant aneurysm regrowth Problems and Tactics A case of giant aneurysm of the internal carotid artery inferior wall presenting regrowth after intial neck clipping was presented. Clinical problems and surgical tactics were retrospectively reviewed. Keywords Giant aneurysm, internal carotid artery inferior wall, clipping, regrowth This 19-year-old, previously healthy woman had experienced a sudden and severe headache and was referred to our department. Computed tomographic (CT) scan did not show the finding of subarachnoid hemorrhage (SAH), but carotid angiograms did reveal two cerebral aneurysms at the intracranial (C1 portion) and cavernous portion of the right internal carotid artery (ICA) (Fig. 7–1). The size of the intracranial aneurysm was ~20 mm in diameter and the aneurysm at the cavernous portion was 8 mm. No neurological deficits or other pathological neuroradiological findings were observed. On angiographic examinations, both the anterior choroidal artery and the posterior communicating artery (PCoA) were found, although the detailed information related to the neck of aneurysm. Filling of the anterior cerebral artery was poor and sufficient cross-flow was not confirmed. Surgical treatment of the intracranial aneurysm was planed, and initially coil embolization was applied;. however, coil-embolization was unsuccessful because of the wide neck of the large aneurysm, and surgical clipping was performed. For the first operation (Fig. 7–2) the patient was placed in the supine position. The right cervical carotid artery was exposed for possible temporary occlusion and for intraoperative angiography. A right frontotemporal craniotomy was performed. After durotomy, the sylvian fissure was widely dissected exposing the ICA aneurysm and surrounding vascular structures. A large semi-fusiform aneurysm was found protruding ventrally of the ICA, located between the origin of the PCoA and near to the ICA bifurcation. The PCoA appeared to originate from the proximal side of the aneurysm body, not from the carotid artery, and the diameter was thicker than speculated on preoperative angiography. At the distal site, the boundary of the neck and body of the aneurysm was clearly visible. The PCoA had eight perforators divided from the origin, and five perforators originating from the carotid bifurcation were identified, but branches divided from the carotid artery, including the anterior choroidal artery, were not observed between the distal site of the aneurysm and the carotid bifurcation. FIGURE 7–1 Right carotid angiograms before (upper) and after (lower) the first operation, showing aneurysms of the C1 segment and cavernous portion of the internal carotid artery. Intracranial giant aneurysm was clipped. (Left) Anteroposterior view. (Right) Lateral view. FIGURE 7–2 Intraoperative view of the internal carotid artery aneurysm before and after clipping procedure. Two fenestrated clips and an added straight one as shown in the schema were applied. The proximal site of the aneurysm (asterisks) was not occluded completely at the origin of the posterior communicating artery. ICA, internal carotid artery; MCA, middle cerebral artery; ACA, anterior cerebral artery.
An Internal Carotid Artery Giant Aneurysm Presenting Regrowth after Neck Clipping
Clinical Presentation
Surgical Procedures and Outcome
First Operation
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 26 A Large Cerebellopontine Angle Arteriovenous Malformation
26 A Large Cerebellopontine Angle Arteriovenous Malformation
 8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
8 Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


