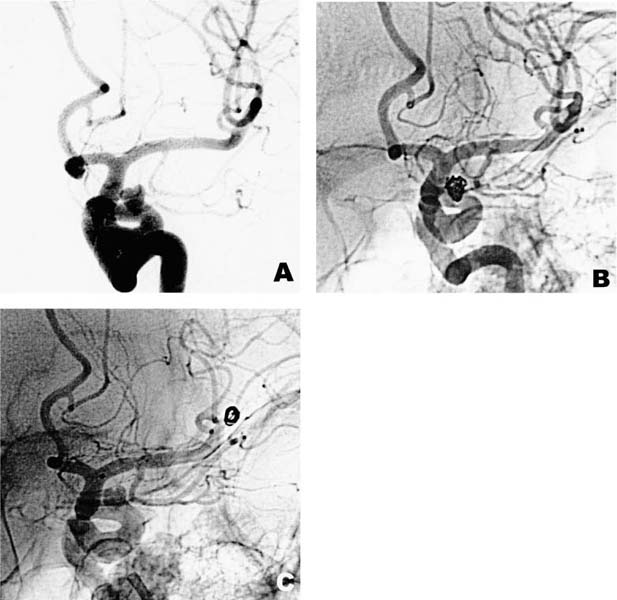
8 Diagnosis Superior wall aneurysm of proximal internal carotid artery Problems and Tactics A patient underwent a Guglielmi detachable coil (GDC) treatment for a small, unruptured aneurysm of the proximal internal carotid artery (ICA). A few hours after the endovascular treatment, the patient developed hemiplegia and aphasia due to migration of the coils causing an occlusion of the M1 segment. An endovascular attempt to retrieve the malpositioned coils failed, resulting in tangling and distal migration of coils into the inferior M2 trunk. The patient underwent emergency surgical recanalization of the inferior M2 trunk by an arteriotomy, with removal of migrated coils, followed by clipping of the unruptured aneurysm. Keywords Internal carotid aneurysm, complication, Guglielmi detachable coil, arteriotomy A 44-year-old man complained of a dull headache. A carotid angiogram showed an unruptured superior wall aneurysm (6 mm) of the proximal ICA on his left side (Fig. 8–1A). The patient requested and underwent intraaneurysmal GDC treatment (Fig. 8–1B). One and a half hours after the procedure, he suddenly developed right hemiplegia and aphasia. An emergency carotid angiogram showed recurrent filling of the aneurysm and migration of the coils causing an occlusion of the left M1 segment. The neurointerventionist attempted to retrieve the coils using a snare catheter but without success, which resulted in tangling and further distal migration of coils into the inferior M2 trunk (Fig. 8–1C). Emergency surgery was necessary to recanalize the occluded vessel and restore the cerebral blood flow. The patient was placed in the supine position, with his head fixed in a three-pin clamp. A standard pterional craniotomy was fashioned on the left side to expose a wide angle to allow for the clip-applying forceps and other microsurgical instruments. As the patient was heparinized during and after the endovascular procedure, the incised margin of the dura was everted and pulled over a sponge with traction stitches to minimize epidural bleeding and to prevent blood from dripping into the field. A slack brain allowed for wide opening of the sylvian fissure to expose the left middle cerebral artery and the ICA. FIGURE 8–1 Left carotid angiograms showing (A) a superior wall aneurysm of the proximal internal carotid artery, (B) Guglielmi detachable coil (GDC) in the aneurysm, and (C) migrated GDC occluding the inferior M2 trunk. Tangled coils were seen through the arterial wall of the distal inferior M2
Emergency Recanalization of the Inferior M2 Trunk by Arteriotomy and Retrieval of Migrated Guglielmi Detachable Coil, and Clipping of Superior Wall Aneurysm of Proximal Internal Carotid Artery
Clinical Presentation
Surgical Technique
Related posts:
 28 Dominant Hemisphere Insular Tumor
28 Dominant Hemisphere Insular Tumor
 9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
9 Large Aneurysm of the Internal Carotid Artery Obliterated with Seven Fenestrated Clips under Intraoperative Monitoring of Anterior Choroidal Arterial Blood Flow Insufficiency
 20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
20 Collateralization via Vasa Vasorum: A Determinant of Therapeutic Efficacy of Coil Embolization of the Thrombosed Giant Aneurysm of the Vertebral Artery
 41 Olfactory Neuroblastoma with Brain Invasion
41 Olfactory Neuroblastoma with Brain Invasion
 45 Clinoidal Meningioma Encasing the Internal Carotid Artery
45 Clinoidal Meningioma Encasing the Internal Carotid Artery
 70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
70 Fibrous Dysplasia of the Paranasal Sinuses and Anterior Cranial Base
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


