To diagnose the cause for falls, first determine whether falls are due to acute loss of brain activity/perfusion or to a balance problem.
Falls are often due to impairments in multiple physiologic systems affecting balance.
Damage to different systems underlying balance control results in different, context-specific instabilities.
Effective fall prevention requires an assessment of contributing intrinsic and extrinsic factors.
Refer patients to multidisciplinary resources early to prevent future falls.
The clinical problem of falls is complex and requires an especially thorough history and comprehensive physical examination of the patient. Although patients with neurologic disorders are particularly prone to injurious falls, many other diagnoses and environmental factors also contribute to falls. When a complaint of falling is presented, the clinician must be prepared to consider a broad differential diagnosis. This chapter will review epidemiologic factors about falls, present a practical approach to discover the correct diagnosis, and discuss how different underlying constraints on balance control can contribute to falls, even when patients have the same diagnosis. Treatment options to prevent future falls, including recommendations on when a referral should be made to a neurologist, will be highlighted.
DEFINITION
The World Health Organization defines a fall as “An event, which results in a person coming to rest inadvertently on the ground or other lower level.” While this definition may seem so intuitive that defining it is redundant, Tinetti et al. (1997) offered an alternative definition that has become widely accepted because it acknowledges that many falls are secondary to other phenomena, not necessarily just a balance problem. Tinetti’s definition of a fall is “A sudden, unintentional change in position causing an individual to land at a lower level, on an object, the floor or the ground, other than as a consequence of sudden onset of paralysis, epileptic seizure, or overwhelming external force.” Illustrating this concept further, one can consider two broad categories of falls: (a) sudden loss of postural tone and/or consciousness (collapsing) and (b) loss of balance (falling like a tree), or failure to recover equilibrium. This distinction represents an important initial branch point in diagnosing pathologies related to falls, and it would be best to consider patients in these categories separately. Those who fall because of loss of balance will be the main focus of this chapter.
SCOPE OF THE PROBLEM
Falls are typically a problem that increases with aging. It is estimated that about 30% of community dwellers older than 65 fall at least once each year; for those in facilities, this number is even higher. As a consequence of falling, about 20% of falls result in medical attention for serious injury, approximately 10% resulting in a bony fracture. The economic cost of falling in the United States is estimated to be 19 billion dollars in total direct costs annually. In the year 2000, 10,300 falls resulted in a fatality in the United States, illustrating the seriousness of this highly prevalent problem. While it has been determined that the economic burden of falls is substantial, falls also lead to reduced quality of life, as immobility, loss of recreational activities, social isolation, and fear of falling are common after falling.
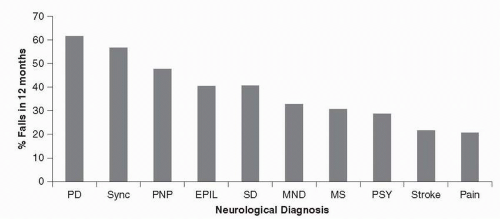
FIGURE 21.1 Fall incidence in neurologic patients by diagnosis. PD, Parkinson disease; Sync, syncope: PNP, peripheral neuropathy; EPIL, epilepsy; SD, spinal disorders; MND, motor neuron disease; MS, multiple sclerosis; PSY, psychogenic. (From Stolze H, Klebe S, Zechlin C, et al. Falls in frequent neurological diseases: prevalence, risk factors and aetiology]J Neurol. 2004;251:79-84, with permission.
▪SPECIAL CLINICAL POINT: Falls in patients with neurologic disorders are three to five times more common than in age-matched people without neurologic diagnoses.
This statistic is not surprising, since balance control involves many parts of the nervous system, and impairments of balance control are a leading cause of falls. Some neurologic diagnoses are more associated with falls and fall injuries than other diagnoses, suggesting that they impair neural areas more critical for balance control. For example, Figure 21.1 shows the relative percentage of patients with falls in the previous 12 months for 489 inpatients admitted to a neurology ward. Patients with Parkinson disease (PD) showed the most falls, with syncope and peripheral neuropathy the next most common causes of falls.
Severity of neurologic disease is related to fall incidence, but not linearly. Early in neurologic disability, falls increase with the amount of neurologic damage. However, as the neurologic disability leads to immobility, patients who are confined to wheelchairs and beds fall less often. For example, patients with amyotrophic lateral sclerosis or severe stroke may not fall because they cannot stand or walk independently, whereas a person with mild PD who continues to ski may sustain a severe fracture from a fall. Thus, frequency of falls should always be considered in relationship to how mobile and active a patient engages in activities of daily living, sports, and outdoor activities.
RISK FACTORS
Many studies have examined risk factors leading to increased falling. It is useful to consider these factors as intrinsic or extrinsic. Examples of intrinsic factors include muscle weakness, balance dysfunction, cognitive impairment, orthostasis, gait abnormalities, mobility limitations, decreased functional status, and a history of previous falls in the last year. Increasing age, especially those 80 or older, use of an ambulatory device, such as a cane or walker, arthritis (especially of the feet), and depression are also associated risk factors. Table 21.1 summarizes how much various risk factors increase the chance of falling in a large cohort of older people.
Extrinsic factors are derived from the external environment, or risky behaviors.
▪SPECIAL CLINICAL POINT: An often overlooked extrinsic factor is polypharmacy, with five or more medications significantly increasing risk of falls in the elderly.
Psychotropic medications such as benzodiazepines, antipsychotics, antidepressants, as well as antihypertensives and anticonvulsants are especially associated with falling. Another important extrinsic risk factor is an unsafe environment, especially throw rugs, stairs, dark areas, and clutter or other obstacles. Behaviors, such as climbing ladders, working on roofs, and sports participation, especially skiing, also increase fall risk. The importance of a particu lar extrinsic factor in increasing the risk for falling for individual patients will depend upon their specific type of balance problem. For example, a patient who shuffles when walking will be at particular risk of falling on throw rugs, a patient with leg weakness or knee joint impairments will be at particular risk on stairs, and a patient with multisensory deficits may be at particular risk of falling in the dark or on an unstable surface.
TABLE 21.1 Ratios of Increased Fall Risk Associated with Various Intrinsic and Extrinsic Factors in the Elderly
a Especially sedatives, antidepressants, pain medications.
DIAGNOSING THE CAUSE OF FALLS
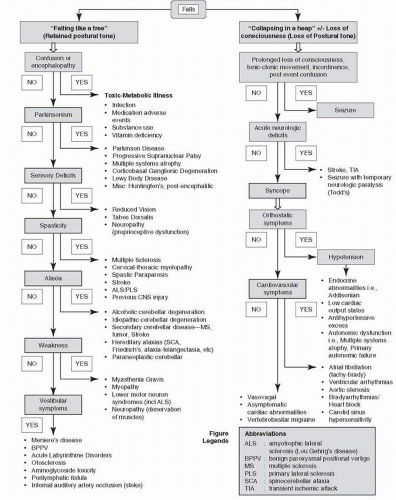
The complaint (often from family members) that the patient is falling should prompt investigation by clinicians, both neurologists and non-neurologists. The broad differential can be intimidating, and the following flowchart (Fig. 21.2) can help navigate the important branch points. While it is often suggested that determining if loss of consciousness has occurred in association with the fall is critical, this point may be unclear in the patient’s mind and even by observers. While recognizing the limitations of this line of questioning, it can help to ask whether the falls appear “collapsing” in nature or not. Often collapsing and impaired consciousness go together, and can indicate low cerebral blood perfusion or seizure, as shown in the right half of the flowchart.
FIGURE 21.2 Flowchart for approach to a falling patient
If impairment of alertness appears to underlie a fall, further signs or historical points should be sought, including tonic-clonic or other rhythmic movements at the time of the fall, nystagmus, prolonged postevent confusion, or incontinence which could indicate seizure activity. If not, then stroke should be ruled out by assessing for new neurologic deficits, keeping in mind that occasionally a seizure can be accompanied by a temporary period of apparent weakness known as a Todd’s paralysis. Once a stroke or seizure is ruled out, then syncope becomes the top consideration. If evidence of orthostasis is found by history or by examination, further investigation of blood pressure instability follows. Frequently, antihypertensive medication excess contributes to this problem, but endocrine deficiencies or autonomic dysfunction can also be causative. Autonomic dysfunction, for example, may result in postural hypotension that can lead to collapsing falls when patients attempt to quickly rise from sitting or lying positions. If no sign of orthostasis is evident, then cardiovascular causes of syncope need to be considered, which may require a cardiology specialty referral. At times, no cardiovascular causes can be identified, and rarer conditions including vertebrobasilar migraine may need to be considered. At this point, a neurologic consultation is warranted for the evaluation of these more unusual conditions.
Sometimes falls are a sign of underlying medical illness or an acute side effect of medications like sedative hypnotics, anticonvulsants, antihistamines/anticholinergics, or substances like alcohol. When falls are due to medication side effects, confusion or encephalopathy is a useful feature to recognize, and the expectation is that these falls will resolve when the illness has been treated or offending medication removed.
So far, this section has focused on the right half of the flowchart, which can be considered as the approach to acute global deficiencies of brain perfusion or electrical maintenance. The bulk of this chapter will now focus on the left half of the flowchart, which can be classified as the approach to falls due to balance maintenance problems. These types of falls are typically more chronic in their temporal course and often, though not always, associated with neurologic conditions. An examination focused on the neurologic system can help place the patient in broad categories that will lead to an accurate diagnosis and treatment plan.
ParkinsonismExamination findings of restpredominant tremor, muscular rigidity, and slowness of movement (bradykinesia) signal parkinsonism, which is a manifestation of an abnormally functioning basal ganglia. Subjectively, patients experience parkinsonism as tremulousness, muscular stiffness, and slowness. Falling is associated with parkinsonism because rigidity and slowness of movement impair balance responses and because many important postural systems are directly affected. A number of diagnoses are characterized by parkinsonism. As the disease advances, cognitive deficits can also contribute to the accumulation of balance constraints.
The most common cause of parkinsonism is Parkinson disease. PD is clinically diagnosed and considered probable if two out of three cardinal signs are present. These signs include rest-predominant tremor, bradykinesia (slowness of movement), and rigidity during passive motion of the limbs or neck. Postural instability is also very common, though not at the beginning of the disease course. Indeed, postural stability deficits usually develop in the middle to later phases of the disease, occurring at least a few years after other parkinsonian symptoms develop.
▪SPECIAL CLINICAL POINT: Early falls are considered a red flag indicating an alternate parkinsonian diagnosis.
While PD accounts for the majority of cases of parkinsonism, the second most common cause is progressive supranuclear palsy (PSP). PSP is important in the context of this chapter because a hallmark feature of the disease is early falling and may be the main symptom presented to the medical provider’s attention. Falls are typically backward in direction, as opposed to PD, where patients typically fall forward. Other symptoms include stiff axial musculature, restricted voluntary ocular excursions, particularly in the vertical downward direction, spastic-ataxic speech, dystonic facial features, and cognitive deficits that are frontal executive in nature.
Other less common conditions that may present with parkinsonism include multiple systems atrophy (MSA) and corticobasal ganglionic degeneration (CBGD). In MSA, combinations of parkinsonism, ataxia, autonomic dysfunction, and pyramidal tract findings can occur. In CBGD, apraxia, cortical sensory disturbance, dystonia, myoclonus, and rigidity present in a usually very asymmetric pattern of onset. Other conditions that also may be considered include fragile × premutation tremor-ataxia syndrome, drug-induced parkinsonism, normal pressure hydrocephalus, and Lewy body disease. If any type of parkinsonism is suspected, a referral to a neurologist or movement disorders specialist is highly recommended. It is important to recognize that several drugs prescribed by nonneurologists are dopamine receptor blockers and can cause drug-induced parkinsonism. These agents (see Chapter 12) include antipsychotic agents, reserpine, and metoclopramide.
Spasticity This problem occurs as a result of damage to the motor tracts originating anywhere from the motor cortex down to the spinal cord before the anterior horn cell (lower motor neuron of the spinal cord). Spasticity is the excessive tonic stretch reflex that is detected in a limb with velocity-dependent maneuvers and is sometimes described as having a “clasp-knife” character. Subjectively, it may be experienced as a stiffness or tightness in the involved muscles and can be associated with painful cramping. As a practical illustration, one may see this as the tightness of muscle tone greater in the extensor and adductor muscles of the legs, causing foot inversion, toe pointing, and even curling in a patient with multiple sclerosis (MS).
Spasticity can lead to falls by a number of mechanisms. Simple reasons may include weakness of involved muscles because weakness often accompanies spasticity as part of an upper motor neuron syndrome (though not always). Another reason for falls with spasticity may be the abnormal posture of a foot, which results in a limited base of support for balance and leads to missteps and tripping while walking. Excessive muscle tone can interrupt the normal coordinated swing cycle of walking and results in weak postural responses and inflexible postural tone with delayed postural latencies. Acute spasms of muscles can add unpredictable instability during stance or gait.
Ataxia Ataxia is the result of hypermetric, poorly coordinated body movements with poor motor learning associated with abnormal cerebellar function. Ataxia can be inherited as a number of conditions, or can be acquired as a result of injury or damage to brain structures responsible for coordination. Clinicians may perceive ataxia in the common broad standing base that compensates for the effects of excessive involuntary body motions that disrupt equilibrium. Damage to the anterior lobe of the cerebellum results in excessive hip and trunk motion during stance and ataxic gait involving inconsistent variable positioning of the feet. When the cerebellar hemispheres are involved, ataxia includes the limbs with similar inaccurate, hypermetric, jerky, and poorly controlled purposeful movements. Ataxia leads to falls for many reasons: poor coordination of stepping, loss of righting mechanisms, hypermetric postural responses, and unstable gait with head motion. Depending on the cause of ataxia, somatosensory, visual, and/or vestibular disruptions may also contribute, as may executive deficits.
The inherited causes of ataxia include autosomal dominant, recessive, and X-linked conditions. Spinocerebellar ataxias are a group of genetically determined conditions that may have associated features such as neuropathy, cognitive dysfunction, parkinsonism, eye movement abnormalities, and other diverse neurologic signs. Other inherited ataxic syndromes have been identified and a thorough family history is important to explore, including mental retardation, as a recently described condition called fragile × tremorataxia syndrome especially affecting older males can be found in families where fragile × syndrome has been diagnosed. If an inherited cause is suspected, a referral to a neurologist or medical geneticist is warranted.
Acquired causes of ataxia can include toxic exposures like alcohol or anticonvulsants, paraneoplastic conditions accompanying cancers of the lung or gynecologic organs for example, structural abnormalities or infections, vitamin deficiencies, and autoimmune conditions such as MS. Idiopathic conditions like MSA or cerebellar degeneration may present with falls early in the course of the disease.
While cerebellar abnormalities can lead to ataxia, disruptions in sensory systems can also result in a similar appearance of ataxia. Neuropathy, especially when proprioceptive function is severely disturbed, or some vestibular disorders can result in unsteadiness of stance and gait that resemble ataxia and result in falls.
Vestibular System Disorders The vestibular system is a bilateral, reciprocal sensory system that contributes to balance control by sensing position and velocity of head motions, as well as gravity. It is useful to consider peripheral vestibular disorders in three broad groupings, those with (a) chronic unilateral or bilateral loss, (b) fluctuating or intermittent dysfunction, and (c) mechanically based vestibular dysfunction. Falls due to vestibular dysfunction can be due to any of the following components including unstable gait with head motion, asymmetric limits of stability, poor sense of the vertical, and loss of sensory feedback.
Examples of chronic or permanent loss of vestibular function include otosclerosis, stapedectomy, acoustic neuroma, aminoglycoside or other ototoxicity, vertebrobasilar stroke, or rarely a unilateral internal auditory artery occlusion leading to a stroke of the vestibular end organ. Menière disease is a classic example of fluctuating vestibular dysfunction, though it may lead to a chronic pattern in later disease. Mechanically based dysfunction of the semicircular canals or otolith organs include benign paroxysmal positional vertigo (BPPV) in which otoconia become displaced from the otoliths and float in the canals, and perilymphatic fistulas or holes in the round or oval windows.
Patients with vestibular deficits may have very poor control of balance, complaints of dizziness, and abnormal eye movements, but not frequent falls. Falls can often be avoided in patients with vestibular injuries because they increase their dependence on vision and somatosensory function using central compensation processes. However, if patients with bilateral loss of vestibular function or with uncompensated unilateral loss of vestibular function find themselves in a dark environment standing on an unstable surface, they may fall “like a tree” without making automatic balance responses because of spatial disorientation from lack of sensory information about their body equilibrium. This “context-specific instability” is often missed when evaluating vestibular loss patients in a well-lit clinic on a firm surface.
WeaknessWhile weakness is common when in conjunction with other neurologic findings such as spasticity in upper motor neuron syndromes, or atrophy of muscles associated with neuropathy, there are syndromes of lower motor neuron, pure muscle disorders, and neuromuscular junction dysfunction where weakness is singularly dominant. Muscle disease including endocrine, inflammatory or toxic myopathies, inclusion body myositis, or neuromuscular junction diseases such as myasthenia gravis can present with varying degrees of weakness and falls. Less common lower motor neuron diseases such as polio, or spinal muscular atrophy can lead to profound weakness especially of the lower extremities. Weakness of muscle activation causes falls because of inability to sustain strength against the pull of gravity and inability to generate adequate, quick increases in force between their feet and the ground to recover equilibrium with automatic balance responses.
TABLE 21.2 Examples for How Each Neurologic Disease is Associated with a Different Set of Constraints on Postural Control