Insufficient sleep time and sleep apnea are the two most common causes of excessive daytime sleepiness.
Obstructive sleep apnea is suspected on the basis of snoring and excessive daytime sleepiness.
Obstructive sleep apnea may be associated with significant morbidity related to sleepiness and morbidity/mortality related to its cardiovascular effects.
Taking a good sleep history is a key to diagnosis and the first step to successful treatment of insomnia.
Narcolepsy typically presents in an adolescent/young adult with excessive sleepiness, sleep attacks, and cataplexy.
Destruction of the VLPO system results in insomnia, whereas destruction of the hypocretin system results in narcolepsy (hypersomnolence/sleep attacks and cataplexy). The control of alternating sleep stages (NREM [nonrapid eye movement]/REM [rapid eye movement] cycling) is attributed to interaction between antagonistic aminergic and cholinergic systems in the brainstem. The aminergic and cholinergic systems also are involved in the process of cortical activation of arousal. In addition to the previously mentioned systems, the dopaminergic system is involved in control of alertness as well, especially the ventral tegmental area (A10). Dopaminergic neurons of the VTA but not substantia nigra (SN) are excited by hypocretins, and there is a greater hypocretin innervation of the VTA than SN. Dopaminergic neurons in the ventral periaqueductal gray (PAG) also are activated during wakefulness. The dopaminergic system, including the descending All projection, may be particularly important for sleep disorders accompanied by anomalies of sleep-related motor control (cataplexy and periodic limb movement [PLM] disorder). Circadian sleep rhythm is modulated by the hypothalamic suprachiasmatic nucleus (SCN). The SCN sets the body clock period to approximately 25 hours, with the light and schedule cues (zeitgebers, “time givers”) entraining it to 24 hours. The retinohypothalamic tract conveys light stimuli to the SCN that directly influences its activity. Melatonin has been implicated as a modulator of light entrainment because it is secreted maximally during the night by the pineal gland (hormone of darkness). Thus, the anterior hypothalamus may serve as a center for “sleep switch” under the influence of the circadian clock.
sleep occurs predominantly in the first third of the sleep period (Fig. 10.2).
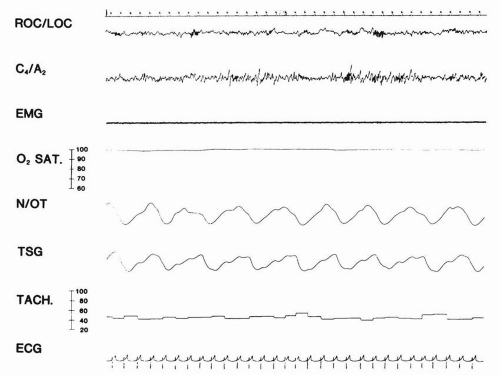 FIGURE 10.1 A typical eight-channel polysomnogram recorded from a normal adult man in stage 2 of nonrapid eye movement sleep. Electro-oculogram (ROC/LOC) recorded from right outer canthus referred to left outer canthus; electroencephalogram (EEG) (C4/A2) recorded from the right central lead referred to the right mastoid; electromyogram (EMG) recorded from the submental musculature; arterial oxygen saturation (O2SAT) transduced by an ear oximeter; nasal and oral airflow (N/OT) recorded by a thermocouple mounted in a plastic respiratory mask; thoracic movement (TSG) recorded by a strain gauge; heart rate recorded by a cardiotachometer; electrocardiogram (ECG) recorded from V5 referred to the left mastoid. |
that the percentage of time spent in each stage varies with age and sex. Figures 10.1 and 10.2 represent a sleep PSMG and architecture plot from a normal adult.
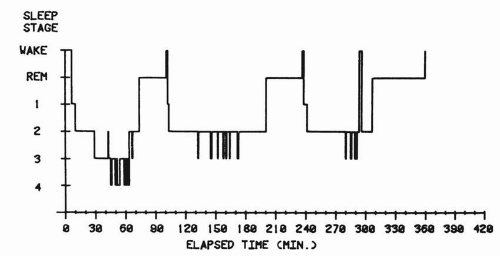 FIGURE 10.2 The sleep architecture of a normal adult man. The progression of electroencephalogram (EEG) stages of sleep demonstrates a concentration of stages 3 and 4 within the first half of the sleep period. Episodes of rapid eye movement (REM) sleep occur at approximately 90-minutes intervals, and the majority of REM appears within the latter half of the sleep period. Waking arousals are few. |
as inadequate sleep hygiene, environmental sleep disorder, altitude insomnia, adjustment sleep disorder, limit-setting sleep disorder, food allergy insomnia, hypnotic-dependent sleep disorder, alcohol-dependent sleep disorder, and sleep-disordered breathing are likely to be accompanied by insomnia. Among circadian rhythm sleep disorders, delayed sleep-phase syndrome is associated with a complaint of sleep-onset delay, whereas advanced sleepphase syndrome is accompanied by a complaint of early awakening. In general, the pattern of insomnia may be primarily (a) difficulty falling asleep (sleep-onset delay, sleep-onset insomnia), (b) early morning arousal (premature awakening, terminal insomnia), or (c) premature awakening(s), sleep fragmentation with inability to fall asleep again (sleep-maintenance insomnia).
full rest if they can go to bed late and sleep until midday. This pattern is characteristic (and probably physiological) in late adolescence and early adulthood. A change in lifestyle and a course of chronotherapy at a sleep disorder center can correct this problem. Delayed sleepphase syndrome may also be treated with a morning session of bright light, which may be combined with an early evening dose of melatonin. Similarly, evening exposure to bright light and light restriction in the morning (wearing dark goggles) may be useful in treatment of advanced sleep-phase disorder. Chronotherapy, an individually designed sleep schedule consisting of a gradual sleep-onset time delay until a desired time is reached, may also help patients with irregular sleep-wake patterns, who sleep for short and variable periods throughout the 24 hours. These people have difficulty falling asleep at conventional times because they have napped recently. Shift workers and those who travel frequently across time zones often experience sleep-onset delay (in addition to jet lag) and may also benefit from a combined bright light-melatonin treatment.
require the facilities of a sleep laboratory. Attempts at operant and classic conditioning as aids in treating insomnia also have had some limited success. A widely accepted behavioral modification technique—stimulus control—is especially useful in correcting maladaptive association of arousal with bedtime routine. Other techniques aimed at reducing tension include progressive muscular relaxation and autogenic training.
or three nights is indicated. Sleep induction is related to the rate of drug absorption. Sleep maintenance is related to dosage and half-life. The timing of the intake of the medications is, therefore, important. Hypnotics with longer half-lives (lasting more than 24 hours) show increased efficacy with two or three nights of administration, but they also show increased residual daytime effects. Some benzodiazepines, such as flurazepam, produce persistent long-acting metabolites and cause definite impairment in alertness, motor performance, and cognitive function in the morning. Because of the intrinsic “tapering” effect of compounds with long halflives, rebound and/or withdrawal phenomena appear to be unlikely; when they do occur, such effects are delayed in onset and are relatively mild. However, there is a much higher likelihood of rebound or withdrawal effect after abrupt discontinuation of short-half-life hypnotics, for which dose tapering is appropriate. When the initial therapy is unsuccessful, changing classes of medications may be useful.
TABLE 10.1 Commonly Used Sleep-Promoting Medications | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
that is, the mean plasma concentration will be no higher after multiple days of therapy than after the first day. At the other extreme is a drug such as flurazepam, with its principal active metabolite desalkylflurazepam. This compound has a very long elimination half-life; 2 weeks or more of long-term treatment will be necessary for a steady state to be attained. The rate of drug disappearance following discontinuation after long-term treatment will mirror the rate of accumulation (i.e., the longer the elimination halflife, the more time will be needed for the drug to disappear). A potential benefit of accumulating a benzodiazepine is that persistence of drug at the receptor sites throughout each 24-hour dosing interval increases the likelihood of a daytime anxiolytic effect, a potential benefit for patients with both anxiety and insomnia. For short halflife hypnotics such as triazolam, however, increased daytime anxiety has been reported in some studies, possibly attributable to wide fluctuations in plasma and receptor-site concentrations between doses. Estazolam, a relatively new benzodiazepine, remains effective as a hypnotic for at least 6 weeks of continuous administration at a dosage of 2 mg at bedtime, with no evidence of clinically significant tolerance. It improves sleep latency and total sleep time, reduces the number of nocturnal awakenings, and improves both depth of sleep and sleep quality in adults with chronic insomnia.
treatment of night terrors or severe somnambulism. Benzodiazepine metabolism varies and is largely age dependent. The elimination halflife of diazepam in healthy men may increase threefold to fourfold from 20 years of age to 80 years of age. The elimination of hypnotics is decreased in elderly people who might have a low renal glomerular filtration rate, a reduced hepatic blood flow, and a decreased activity of hepatic drug-metabolizing enzymes. The choice of hypnosedatives for elderly patients with sleeponset delay, especially when they are acutely hospitalized, is complicated by the risk of a paradoxical excitation at nighttime (sun-downing), which may be precipitated or exacerbated by medication. Although diphenhydramine has been useful in many of these patients, there is a risk of increasing their confusion because of its anticholinergic effect. These problems can be minimized by adjunctive measures, such as leaving a light on in the patient’s room, and by frequently reorienting the patient to the unfamiliar surroundings. A family member occasionally may be required to stay with the patient.
“tonic” for sleep, as is chamomile (Marticaria recutita). Several other herbs are used as sleep aids because of their reported sedative effects: gotu cola (Centella asiatica), hops (Humulus lupulus), lavender (Lavandula angustifolia and others), passionflower (Passiflora incarnata), and scullcap (Scutellaria lateriflora). Hepatoxicity was described for scullcap when used in combination with valerian root, but this may have resulted from substitution of a particular herb with species of germander (Teucrium).
1. A sensation of an urge to move the limbs (usually legs)
2. Motor restlessness to reduce sensations
3. Onset or worsening of the symptoms when at rest
4. Marked circadian variation in occurrence or severity of symptoms, with worsening or sole presence of symptoms in the evening.
iron deficiency, pregnancy) associated with iron deficiency also are associated with RLS. Low brain iron may lead to dopaminergic dysfunction, as documented by decreased D2R, decreased dopamine transporter, and increased extracellular dopamine in rats deprived of iron in early life. In some cases, restless legs and PLMs are caused or exacerbated by dietary substances (e.g., caffeine) or medications (e.g., neuroleptics and tricyclic antidepressants).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


