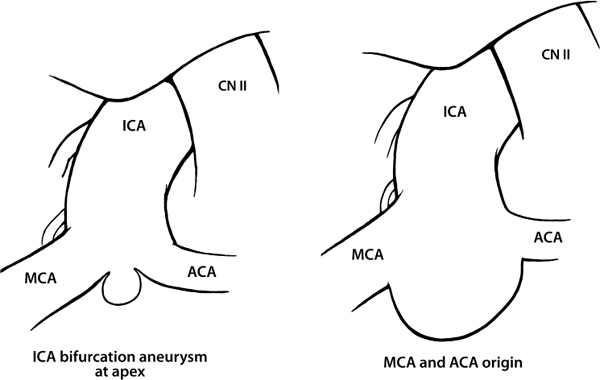
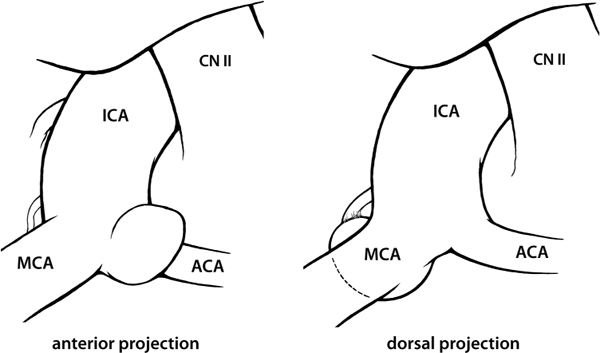
5 These are relatively uncommon aneurysms with a special predilection for occurring in children and adolescents. Both technically and conceptually they have much in common with basilar bifurcation aneurysms, being situated at the terminal apex of the artery at the origin of major large branch arteries and intimately involved with small important perforating vessels on their deep aspect. The carotid bifurcation itself generally occupies the rostral extent of the carotid cistern immediately medial to the origin of the sylvian fissure; elongated, ectatic carotid arteries may extend laterally into the fissure itself, while abnormally short supraclinoid carotid segments may terminate in the posterior portion of the cistern. Internal carotid artery (ICA) bifurcation aneurysms may take origin from the apex alone (small aneurysms with small necks) or from the apex with some involvement of either the proximal A1 or M1 segment (larger aneurysms with broad necks), or they may actually be located exclusively on the very proximal aspect of either main branch (usually small aneurysms). Not infrequently, very small lesions at the A1 origin may only be visible on routine angiographic projections as a double density superimposed on the proximal A1 segment; special views (such as rotational or transorbital oblique projections) may be required to conclusively identify the lesion (Fig. 5.1). Fig. 5.1 Aneurysms of the ICA bifurcation. In addition to the obvious A1 and M1 branch origins, perforating arteries from the carotid bifurcation and the medial aspect of the middle cerebral artery (MCA) may be involved with the aneurysm neck; deep to the aneurysm and hidden by it from the surgeon lies the anterior choroidal artery, a very real potential source of morbidity in the treatment of these aneurysms. While the principal axis of projection for these aneurysms, like those of the basilar bifurcation, is superior, there is a surprising amount of variability in the degree of anterior-posterior tilt (Fig. 5.2). Lesions involving the A1 origin generally project somewhat anteriorly into the overlying orbital cortex, while those of the apex itself or proximal M1 segment may be directed sharply dorsally into the posterior aspect of the carotid cistern. This may result in the aneurysm projecting behind and somewhat medial to the distal ICA when viewed through the microscope. Aneurysms with this posterior projection are frequently intimately involved with the anterior choroidal artery. Fig. 5.2 Projection of ICA bifurcation aneurysms. Prior to selecting a final operative approach the surgeon should carefully evaluate the exact location and projection of the aneurysm and be aware of the size of the contralateral A1 segment, the patency of the anterior communicating artery, the course of the ipsilateral anterior choroidal artery, and the proximity of the lenticulostriate arteries to the M1 origin.
Aneurysms of the Internal Carotid Artery Bifurcation
General
Anatomy
Projection
Procedure
Approach
Related posts:
 The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Vertebral Artery at the Origin of the Posterior-Inferior Cerebellar Artery
Aneurysms of the Proximal Internal Carotid Artery
The Evolution of the Intracranial Aneurysm Surgeon
Operating Room Considerations: Equipment, Setup, and Culture
Surgical Management of Previously Coiled Aneurysms
Aneurysms of the Proximal Basilar Artery
Aneurysms of the Vertebral Artery at the Origin of the Posterior-Inferior Cerebellar Artery
Aneurysms of the Proximal Internal Carotid Artery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


