Answers
1.D. All three are mechanisms of anti-acetylcholine receptor antibodies.
2.B. The medial lemniscus (ML) is widely separated from the anterolateral system (ALS) in the medulla. In fact, ML and ALS fibers receive different blood supplies in the medulla. In the midbrain and pons, the ML and ALS are in close proximity and receive similar blood supplies.
3.D. The CT scan represents sclerosis of the sacroiliac (SI) joint, which may be seen in ankylosing spondylosis. This is representative of the diagnosis of sacroiliitis. Clinically the patient usually presents with SI joint pain and on exam has tenderness along the SI joint with compression as well as a positive thigh thrust and thigh compression exam and a positive flexion, abduction, and external rotation (FABER) test. Pain upon internal rotation of the hip is characteristic of hip joint dysfunction or disease.
4.A. McRae’s line is from the basion to the opisthion.
5.C. It is helpful to remember that this pattern of somatotopy can be appreciated in the descending motor pathways: those that are concerned with flexor musculature (corticospinal tract and rubrospinal tract) lie dorsal to those tracts concerned with extensor musculature.
6.D. Although skin surface fiducial registration is commonly used in brain neuronavigation, it is not very effective in the spine due to the parallax that is seen from registering on the skin and attempting to navigate at the level of the bone, which tends to be significantly deeper than the level of the skin. The other techniques described for localization are effective in identifying the level of interest in that the thoracic spine adequately.
7.A. Rhinocerebral mucormycosis on pathology reveals pleomorphic short and wide nonseptate hyphae. It can be treated with Cancidas, voriconazole, and AmBisome. It may cause hemorrhagic necrosis and ischemic strokes.
8.B. Somatic motor efferents to the sphincter are located in the ventral lateral area of Onuf’s nucleus. Sacral parasympathetics to the bladder are located in intermediolateral cell columns of the sacral cord. Barrington’s nucleus is also known as the pontine micturition center and is responsible for initiating the process of micturition.
9.C. Cerebral ischemia begins when CPP falls below 50 mm Hg.
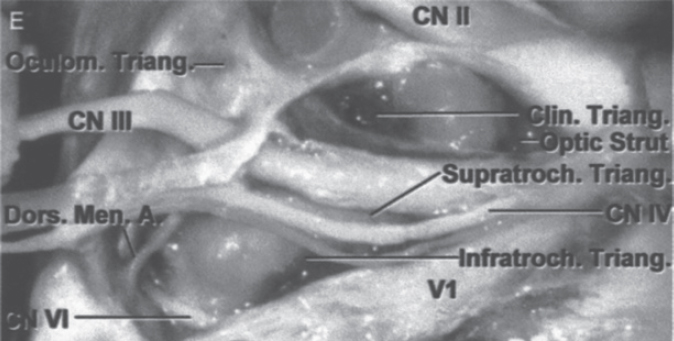
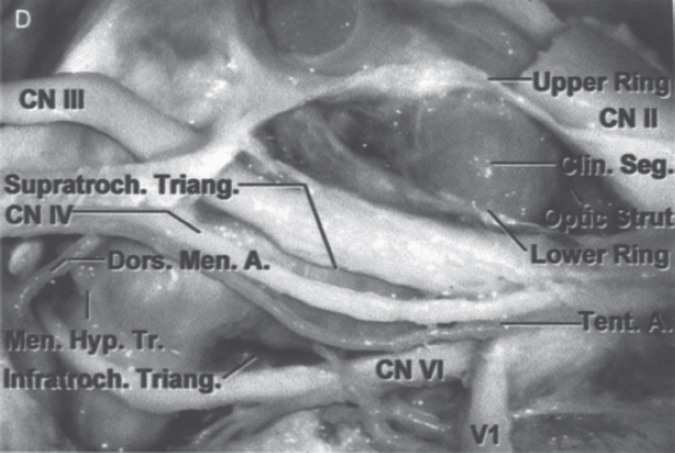
10.B. The clinoidal triangle is defined by the medial border of the optic nerve medially and the oculomotor nerve laterally.
11.E. Dysphagia in myasthenia gravis is fatigable, and the patient often relates a history of little difficulty with breakfast, moderate difficulty with lunch, and inability to eat in the evening.
12.E. Skin changes precede muscle abnormalities in dermatomyositis (DM). Polymyositis (PM) is diagnosed by fibrillation potentials on electromyography (EMG) and elevated creatine phosphokinase (CPK) levels (higher than those for DM). In polymyositis, there is widespread single-fiber necrosis, and T cells with macrophages may be found in the muscle fibers. PM is the most frequent inflammatory myopathy.
13.E. Protein 14-3-3 is elevated in the cerebrospinal fluid (CSF) with destructive diseases of the central nervous system (CNS). This protein is sensitive for Creutzfeldt-Jakob disease, but not specific.
14.B. The posterior cord gives rise to the axillary nerve and the radial nerve as its terminal branches.
15.C. The pterion is located about two fingerbreadths above the zygomatic arch, and a thumb’s breadth behind the frontal process of the zygomatic bone; however, the zygomatic bone does not form the pterion.
16.D. SHH has been found to have the critical roles in development of the limb and midline structures in the brain and spinal cord. Mutations in the human SHH gene cause holoprosencephaly type 3 as a result of the loss of the ventral midline. SHH is secreted at the zone of polarizing activity located on the posterior side of a limb bud in an embryo. The SHH transcription pathway has also been linked to the formation of embryonic cerebellar tumors such as medulloblastoma. SHH has been shown to act as an axonal guidance cue: SHH attracts retinal ganglion cell axons at low concentrations and repels them at higher concentrations. SHH plays a critical role in the induction of the floor plate and diverse ventral cell types within the neural tube.
17.D. After basilar skull fractures, the most common pathogen is Streptococcus pneumoniae, and the infection usually occurs within the first few days.
18.C. The zona incerta is a zone of gray matter between the thalamic and lenticular fasciculi. It is composed of cells that are continuous laterally with the thalamic reticular nucleus. Unlike the thalamic reticular nucleus, the neurons of this zone display immunoreactivity for the calcium binding protein calbindin D-28k. It receives corticofugal fibers from the precentral cortex.
19.A. While lower cranial nerve dysfunction may be a relative contraindication for vagal nerve stimulation, upper cranial nerve deficits do not represent such a contraindication.
20.D.
21.B.
22.E. Weber’s syndrome involves the base of the midbrain. It is characterized by CN III palsy with crossed hemiplegia. All other syndromes mentioned may have ataxia as part of the clinical findings.
23.E.
24.C. Lesions of the dorsomedial nucleus of the thalamus, hippocampus, or temporal cortex cause memory impairment.
25.B. The X-ray shows a cervical rib, usually associated with ulnar nerve weakness and paresthesia, Raynaud’s syndrome, and traction meningocele.
26.E. Bannayan–Riley–Ruvalcaba’s syndrome (BRRS) is a rare overgrowth disorder with occurrence of multiple subcutaneous lipomas, macrocephaly, and hemangiomas. The disease is inherited in an autosomal dominant fashion, but sporadic cases have been seen. The syndrome belongs to a family of hamartomatous polyposis syndromes, which includes Peutz–Jeghers’s syndrome, juvenile polyposis, and Cowden disease. Mutation of the PTEN gene is associated with this syndrome, Cowden disease, Proteus syndrome, and Proteus-like syndrome. These four syndromes are referred to as PTEN hamartoma-tumor syndromes. Intracranial arteriovenous malformations represent a rare feature of BRRS. Capillary malformation or “port-wine stain,” is a cutaneous vascular anomaly that initially appears as a red macular stain that darkens over time. It also occurs in several combined vascular anomalies that exhibit hypertrophy, such as Sturge–Weber’s syndrome and Klippel–Trénaunay’s syndrome.
27.B. The external capsule is located between the claustrum and the putamen. The extreme capsule is located between the claustrum and the insular cortex.
28.B. Serotonin pathways inhibit copulation, explaining the side effect of decreased libido with selective serotonin reuptake inhibitors (SSRIs) used to treat depression. Administration of L-dopa increases libido. Noradrenergic receptors in the brain exert an inhibitory effect on penile erection.
29.E. The peak reduction in intracranial pressure (ICP) occurs in about 15 minutes after administration of mannitol. The duration of action of mannitol is about 4 hours due to the rapid renal elimination of the drug. When mannitol is used with furosemide, the combined effect on ICP reduction is greater than if either were used alone.
30.C. The paramedial triangle (also known as the supratrochlear triangle) is defined medially by the medial border of the oculomotor nerve and laterally by the lateral border of the trochlear nerve.
31.D. The Tensilon test is sensitive in diagnosing a defect in neuromuscular transmission but is not specific for myasthenia gravis (MG). The Tensilon test is especially useful in ocular MG, when other diagnostic tests may be negative. Depending on the mechanism of acetylcholine receptor (AchR) antibodies, there may be insufficient numbers of AchRs available so that a negative Tensilon test does not negate the diagnosis of MG. There is no correlation between the results of the Tensilon test and the subsequent response to pyridostigmine.
32.D. The posterior interosseous nerve (C7, C8) is a branch of the radial nerve. The posterior interosseous nerve innervates the extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris. The extensor carpi ulnaris extends the hand at the wrist joint. This muscle is spared in posterior interosseous syndrome.
33.B. The magnetic resonance angiography scan (MRA) represents the findings of a left anterior frontal arteriovenous malformation (AVM) of which the nidus measures between 3 and 6 cm, which adds two points in the Spetzler–Martin grading system. It is located in noneloquent brain and has superficial drainage; therefore it is a grade 2 Spetzler–Martin AVM.
34.B. Interruption of the inferior geniculocalcarine fibers in the temporal lobe produces a “pie in the sky” deficit (contralateral superior quadrantanopia).
35.D. Ocular myoclonus is a pendular vertical oscillation of the eyes, usually of large amplitude and often occurring with movements of the palate. It can develop months to years after bilateral destructive lesions of the central tegmental tract and is often accompanied by bilateral horizontal gaze palsies and is associated with hypertrophy of the inferior olivary nucleus.
36.A. Early hypoxemia characterizes ARDS.
37.C. Maximum collagen deposition occurs at 42 days (about 6 weeks). Tensile strength keeps on increasing until 2 years.
38.B. Rosenthal fibers are by no means a requisite feature of pilocytic astrocytoma. Rosenthal fibers are composed of alpha B cystallin and are surrounded by intermediate filaments.
39.E. Barbiturates are also thought to stabilize lysosomes, suppress the formation of edema, and reduce intracellular accumulation of calcium. The inverse steal phenomenon involves barbiturate-induced vasoconstriction resulting in shunting of blood from normal brain to relatively ischemic areas.
40.C. Parkinson’s triangle is also known as the infratrochlear triangle.
41.C. The majority of acetylcholine receptor (AchR) antibodies are immunoglobulin G (IgG). Cyclosporine should be used once first-line treatments have failed. Pathological abnormalities of the thymus occur in up to 80% of patients. Weakness confined to the ocular muscles for over 3 years suggests good prognosis.
42.D.
43.E. Tolosa–Hunt syndrome is characterized by ocular and retro-orbital pain, ocular motor paralysis (with papillary sparing), and possibly sensory loss over the forehead with granulomatous inflammation of the superior orbital fissure or the lateral wall of the cavernous sinus. The other conditions described lack an inflammatory response.
44.B. The most accurate description of Wernicke’s area is that it includes the supramarginal (39), angular (40), and posterior one-third of the superior temporal gyri.
45.A. Bursts of back-to-back saccades seen in opsoclonus and ocular flutter may be attributable to a disorder of pause cell modulation of burst cell function.
46.C.
Scan 1 shows a glomus tympanicum tumor, which may be associated with catecholamine release causing hypertension, or serotonin and kallikrein release causing bronchoconstriction, abdominal pain, and explosive diarrhea. Glomus tympanicum tumors may also release histamine and bradykinins during surgery causing hypotension and bronchoconstriction. Scan 2 shows a meningioma of the cerebellopontine angle (CPA), which usually presents initially with facial nerve involvement. Acoustic schwannomas present initially with hearing loss and tinnitus. |
52.A. Disseminated intravascular coagulation (DIC) is most frequently associated with obstetric catastrophes, metastatic malignancy, massive trauma, and bacterial sepsis. The neurosurgeon should be aware that DIC can occur when there is major cerebral tissue injury. The decrease in fibrinogen most closely correlates with increased bleeding. Treatment is by removing the causative agent, heparin, cryoprecipitate, platelets, and whole blood.
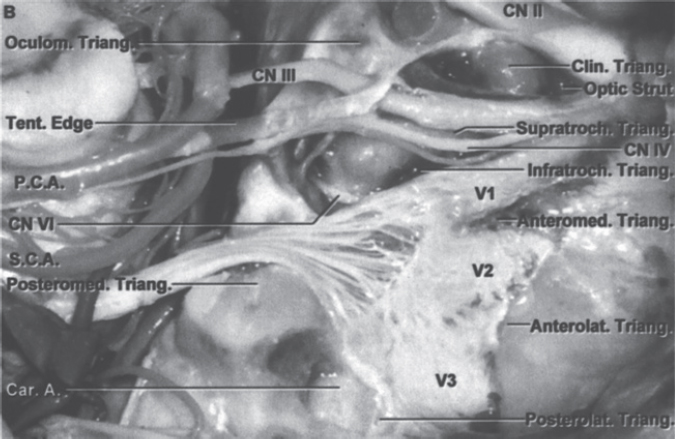
53.C. The mastoid air cells and the posterior middle fossa are innervated by V3. The supratentorial compartment is innervated by V1 and V2. The infratentorial compartment is innervated by IX, X, and C1–C3 posterior roots.
54.D. The band of Gennari divides the fourth layer of cortex into two granular layers with a thick myelin layer. The band is located only in area 17 (primary visual cortex, also known as V1). When Gennari described this in 1782, he had no idea that this or any other region of the visual cortex might be concerned with vision.
55.E. The neural integrator for horizontal eye movements is located in the nucleus prepositus hypoglossi (NPH) at the pontomedullary junction.
56.C. Climbing fiber input is most active at times when the subject is performing new complex movements. The climbing fiber input can modify the synapse between the parallel fiber (from the granule cell) and the Purkinje cell.
57.D. The combination of high trophic hormone and low target hormone indicates target gland failure.
58.D. The opponens pollicis inserts on the first metacarpal bone.
59.C. The MRI with contrast demonstrates a left cerebellopontine angle lesion most consistent with a vestibular schwannoma. Most patients have involvement of the eighth cranial nerve initially. They may also more commonly present with decreased facial sensation or numbness with involvement of the trigeminal nerve; however, facial nerve involvement with a tumor of the size shown is relatively uncommon.
60.B.
61.C.
62.A.
63.E.
64.D.
65.C. The medial longitudinal fasciculus (MLF) is responsible for the binocular coordination of all categories of horizontal, vertical, and oblique eye movements with the exception of vergence movements. Upbeating nystagmus on upgaze is a feature of MLF lesions.
66.C. Both Apert’s and Crouzon’s syndromes are autosomal dominant (both may also be sporadic). Both are associated with bilateral coronal synostosis. Patients with Apert’s syndrome manifest more severe mental retardation than patients with Crouzon’s syndrome.
67.E. In addition to stimulating the synthesis and secretion of thyroid stimulating hormone (TSH), thyrotropin-releasing hormone (TRH) is a potent secretagogue for prolactin, and to a lesser extent adrenocorticotropic hormone (ACTH), and growth hormone (GH).
68.C. The metacarpophalangeal joint of the ring finger is flexed by the lumbrical, palmar, and dorsal interosseous muscles, which are innervated by the ulnar nerve. The joint is extended by the extensor digitorum, which is innervated by the radial nerve. The median nerve is mainly involved with flexion of the ring finger.
69.E. Profile expression:
Survivin—83%
MMP-9—69%
EGFR—63%
MDM2—31%
Fas (APO-1/CD95)—100%
70.D.
71.E. Serum concentration of prolactin (PRL) is increased after tonicoclonic seizure activity but is not affected by nonepileptic seizures.
72.D. The subfornical organ is located on the inferior surface of the fornix at the level of the foramen of Monro.
73.A. The sinuvertebral nerve arises just distal to the dorsal root ganglion. The posterior disk receives its innervation from the sinuvertebral nerves. The anterior disk receives its innervation from the gray rami communicans.
74.B. Repetition is impaired in conduction aphasia.
75.B. The usual diameter of the internal cerebral artery at the clinoid area is about 8 mm. This aneurysm is slightly smaller than the artery’s diameter.
76.C. The Torg-Pavlov ratio is a measure of cervical spinal stenosis and is the ratio of spinal canal to vertebral body. A normal cervical spinal canal will have a ratio of about 1.0. A stenotic cervical canal has a ratio of <0.8.
77.B. Primary glioblastoma has an incidence that is about 10 times higher than secondary glioblastoma. The mean age at presentation in secondary glioblastoma is much younger (45 years) than in primary glioblastoma (62 years). Primary glioblastoma is more common in males when compared to secondary glioblastoma. The median survival at presentation is longer in secondary glioblastoma as compared to primary glioblastoma. Loss of heterozygosity on 10p or 10q is one of the most common genetic mutations in primary glioblastoma.
78.C. The medial brachial cutaneous nerve (from the medial cord) contains sensory fibers that have cell bodies in the dorsal root ganglia. It also contains sympathetic postganglionic fibers that have cell bodies in the sympathetic chain ganglia.
79.B. The perforant path is the main excitatory pathway to the hippocampus. When perforant path fibers are stimulated, histological changes develop in the pyramidal nerve cells of CA1 and CA3.
80.D.
81.B. Up to 80% of the population will experience a tension headache in their lifetime. Amitriptyline is the most effective medication used to prevent tension headaches.
82.C. The ambient cistern contains the trochlear nerve.
83.B. The anterior and medial scalene muscles insert onto the first rib, and the subclavian artery, subclavian vein, and brachial plexus pass between them.
84.A. Pure word blindness is characterized by alexia without agraphia. The patient is unable to read but is able to understand speech, write, and speak. It is caused by a lesion of the left geniculocalcarine tract and the corpus callosum.
85.C. Preventing seepage of blood into the ventricular system during a hemispherectomy is accomplished by obstructing the foramen of Monro and maintaining the integrity of the septum pellucidum.
86.A. Experiments in functional physiology defined a limited role of the horizontal fibers and reinforced the anatomical principles of vertical columnar organization in the cortex. This functional columnar organization of cortical architecture is the key principle in multiple subpial transection.
87.D. Sexual precocity is often the presenting symptom of hypothalamic hamartomas. Hamartomas may also cause gelastic (laughing) seizures.
88.D. Pleomorphic xanthoastrocytoma (PXA) is an astrocytic neoplasm with a relatively favorable prognosis.
89.B. Excitatory input from CA3 to CA1 pyramidal cells is carried by Schaffer collaterals. These collaterals spare the CA2 region.
90.B. The MRI scan of the lumbar spine demonstrates a far lateral foraminal disk herniation at L4–L5 on the left side. Most likely, the L4 nerve root will be involved and the patient will present with weakness of the tibialis anterior and decreased sensation along an L4 distribution in the left lower extremity.
91.B. Although a midline laminotomy or laminectomy may be employed for decompression and removal of the disk it is often more effective to approach the disk via a direct approach that is paramedian with a partial facetectomy in order to remove the foraminal and extraforaminal portions.
92.D. The gracile and cuneate fasciculi are supplied by the posterior spinal arteries. The paired posterior spinal arteries (arising from either the posterior inferior cerebellar artery (PICA) or vertebral artery) supply the posterior one-third of the spinal cord.
93.C. Adson’s test is used in the examination of thoracic outlet syndrome. In this example the examiner is checking to see if the radial pulse is obliterated. Compression of nerves causes wasting of muscles supplied by the lower trunk of the brachial plexus.
94.E. The corticobulbar tract is located in the genu of the internal capsule.
95.D. The medial forebrain bundle traverses the entire lateral hypothalamic area and interconnects the septal area and nuclei, the hypothalamus, and the midbrain tegmentum. The medulla is connected with the hypothalamus via the dorsal longitudinal fasciculus, which projects to the parasympathetic nuclei of the brainstem.
96.D. It is postulated that the closure of the lambdoid sutures, common in Crouzon’s syndrome, results in cerebellar tonsillar herniation.
97.A. The most severe forms of hypothalamic cachexia are seen in lesions of the lateral hypothalamus.
98.C. Lesions of the prefrontal cortex result in a failure to discriminate odors. The prefrontal cortex receives projections from the pyriform cortex. There is also a projection from the pyriform cortex to the dorsomedial thalamus to the prefrontal cortex.
99.A. The amino acids phenylalanine and tyrosine are precursors for catecholamines (dopamine, norepinephrine, epinephrine).
100.D. Renal cell carcinoma has a predilection to the ventricular system.
101.B. The majority of cases of glioblastomas are primary that develop without clinical or histological evidence of a less malignant precursor lesion. They occur primarily in the elderly and typically present genetically with loss of heterozygosity 10q, EGFR amplification, p16INK4a deletion, and PTEN mutations. Secondary glioblastomas occur through progression from low-grade diffuse astrocytoma or anaplastic astrocytoma and tend to present in younger patients. TP53 mutations are the most frequent in the pathways to these tumors being often present in precursor low-grade astrocytomas.
102.B. The straight sinus is formed by the great cerebral vein (of Galen) and the inferior sagittal sinus.
103.D. Oscillopsia is a condition where objects seem to wiggle; it sometimes accompanies downbeat nystagmus.
104.A. Atropine blocks only muscarinic receptors, thus only preganglionic synapses are affected.
105.A. Wernicke’s encephalopathy is due to deficiency of thiamine (B1).
106.D. Gustatory fibers of the solitary nucleus terminate in the VPM. Fibers carrying thoracic information travel via solitary tract and terminate in the parabrachial nucleus and hypothalamus.
107.B. In contrast to diffuse astrocytomas, anaplastic astrocytomas typically display mitotic activity.
108.D. The typical site for a cavernous hemangioma of the orbit is in the intraconal space lateral to the optic nerve.
109.D. HIV-infected individuals have an increased risk of cerebrovascular incidents associated with intravenous drug abuse, low CD4 cell count, and exposure to abacavir, but not with HAART. A CD4 cell count ≤ 200 cells/mL prior the start of HAART increased the risk of cerebrovascular events.
110.E. Arteries from the ependymal surface feed the arteriovenous malformation (AVM).
111.A. Under conditions of neuronal activation, dopamine beta-hydroxylase is the rate-limiting step. However, under basal conditions tyrosine hydroxylase is the rate-limiting step.
112.B. The venous angle is a landmark of the foramen of Monro. It is formed by the union of the septal vein and the terminal (also called thalamostriate) vein.
113.E. Ocular bobbing is a rapid downward movement of the eyes with a slow return to midposition and has many causes.
114.E. This CT scan reveals dense sclerosis around a lytic lesion with a central calcified nodule in the lumbar neural arch consistent with osteoid osteoma.
115.C. The striae medullares (rhombencephali) arise from the arcuate nuclei of the medulla and are seen on the floor of the rhomboid fossa. These fibers divide the rhomboid fossa into a rostral pontine half and a caudal medullary half. The stria medullaris (thalami) contains septohabenular fibers. The stria terminalis is a semicircular fiber bundle extending from the amygdala to the hypothalamus and septal area.
116.C. No blood vessels penetrate the intervertebral disk. Delivery of nutrients is entirely dependent on diffusion.
117.D. The olivocochlear bundle arises from the region of the superior olivary nucleus and projects contralaterally back to the hair cells of the cochlea. Stimulation of this bundle results in inhibition or reduction of responses of auditory signals by auditory nerve fibers.
118.B. Pleomorphic adenomas of the lacrimal gland should be removed with a cuff of normal tissue to reduce the risk of tumor seeding and recurrence. An incisional biopsy should not be performed on this type of tumor.
119.C.
120.C.
121.C. Hydromyelia has ependymal lining. It can be associated with both hydrocephalus and Chiari but can also be postmeningitic and associated with tumors. It can be either communicating with the fourth ventricle or just isolated and noncommunicating. Syrinxes on the other hand lack any ependymal lining.
122.B. The superior cerebellar artery supplies the superior surface of the cerebellum and the cerebellar nuclei.
123.D. In the comatose patient, a lesion at the level of the vestibular nuclei results in extensor movements of the arms and weak flexor movements of the legs. Flaccidity of the lower and upper extremities occurs with lesions below the vestibular nuclei. Lesions above the red nucleus (decorticate) result in flexion of the upper and extension of the lower extremities. Lesions below the red nucleus (and above the vestibular nuclei) result in extensor posturing of all extremities (decerebrate).
124.E. Fibers of the chorda tympani reach the sphenopalatine ganglion to produce “crocodile tears,” also known as Bogorad’s syndrome.
125.A. With a cervical syrinx, one would expect attenuation or abolition of the cervical N13 evoked potential. N13 attenuation may be due to involvement of those laminae of the dorsal horn that receive input from large-diameter mechano-receptor fibers.
126.C. Wolff’s law states that a bone develops the structure most suited to resist the forces acting upon it. Sherrington’s law: every posterior spinal nerve supplies a special region of skin. Jackson’s law: the nerve functions that are latest developed are the first to be lost. Delpech’s principle: in spondylolisthesis, when slippage reaches around 30% the anterior inferior part grows at a faster rate than the overloaded posterior part of the vertebral body. Flourens’ law deals with nystagmus, not spine biomechanics.
127.D. Chordomas tend to be in the midline, whereas chondrosarcomas are more frequently found off the midline (at the petrosphenoid synchondrosis). Chordomas express S-100 only variably. Normal neurological examinations are more common in patients with chordoma, whereas visual loss, facial numbness, and multiple cranial neuropathies are more common in patients with chondrosarcoma. These differences probably reflect the tendency of chordomas to originate from the clivus and chondrosarcomas from the temporal bone.
128.A. Thalamotomy is quite effective for medically refractory essential tremor. The Parkinson’s patients who benefit most from thalamotomy are usually young, with tremor-predominant Parkinson’s disease.
129.D. Due to considerable variation in the attachment of the dentate ligament, the best estimate of the equator is the midway point of the dorsal and ventral rootlets. The equator is a useful landmark for the posterior extent of a cordotomy incision and marks the point of the sacralmost fibers of the spinothalamic tract. The exiting ventral root is about 5 mm from the anterior spinal artery.
130.C. It usually takes 12 to 18 months for radiation changes to appear on MRI scans.
131.C. L-dopa is converted very quickly to dopamine by aromatic L-amino acid decarboxylase (AADC). Dopamine is converted to norepinephrine (NE) by dopamine beta hydroxylase, which is found in vesicles within the catecholaminergic neuron.
132.B.
133.A. The length constant is the distance along a fiber where a change in the membrane potential produced by a given current decays to a value of approximately one-third of its original value. It is directly proportional to membrane resistance and inversely related to axial resistance (the resistance of the cytoplasm within the fiber).
134.D. Raynaud’s phenomenon is caused by mast cell dysfunction; sympathectomy has not proven helpful. Half of these patients have collagen vascular disease.
135.D. Epidural hematomas are the most common intracranial hematoma in children. Although an arterial component is of major concern, diffuse oozing from the bone or from the highly vascularized periosteal surface of the dura is now considered to be a more common source of epidural hematomas in children.
136.E. Spondylolysis is a bone defect in the posterior vertebral arch between the upper and lower articular processes, that is, the isthmus or pars interarticularis.
137.B. Winged scapula is caused by paralysis of the serratus anterior muscle as a result of damage to the long thoracic nerve that arises from the roots of the brachial plexus (C5–C7).
138.A. The typical thalamotomy target is the Vim (ventralis intermedius) nucleus. Often just inserting the electrode into Vim reduces the tremor (microthalamotomy effect), and indicates that the electrode is in a good position.
139.D. All are derived from the telencephalon.
140.D.
141.E. The MRI represents thoracic diskitis at a midthoracic level. Oftentimes this can be treated medically. Indications for surgery, however, do include failure of medical treatments, requirement for identification of offending agent via biopsy, mass effect caused by compression of the cord, or instability that is caused by an abscess or significant bony destruction. Sensory deficit alone is not a clear indication for surgical intervention.
142.B.
143.D. The spiral ganglion consists of bipolar neurons of the cochlear division of the vestibulocochlear nerve.
144.E. The supplementary motor area (area 6) is unique because a lesion in that location is associated with no language output, usually with complete recovery in weeks to months. This is in contrast with the perisylvian language sites.
145.A. During middle fossa approaches, this anatomy can be appreciated. As the dura is elevated, branches of the middle meningeal artery are encountered, and the greater and lesser superficial petrosal nerves are identified immediately posterior to the foramen spinosum. With careful bone removal, the greater superficial petrosal nerve can be traced back to the geniculate ganglion.
146.E. The position of the posterior inferior tip of L5 above one of the quarters characterizes grade I, II, III, or IV spondylolisthesis, respectively (III–V being higher grades).
147.D. Golgi tendon organs detect tension in the muscle fiber. Afferent signals are carried by Ib fibers to interneurons that decrease the alpha motor neuron output.
148.D. The ventralis intermedius (Vim) is thought to be a relay nucleus for kinesthetic sensation. All observations indicate placement in the Vim. Contralateral paresthesias from stimulation of the Vim occur at higher thresholds than those obtained from the ventralis caudalis (VC) nucleus (posterior to the Vim).
149.C. Glomeruli of the olfactory nerve are composed of mitral and tufted cells. Axons of mitral and tufted cells go on to form the lateral olfactory tract.
150.A. The sylvian triangle is defined angiographically by (1) the most posterior branch of the middle cerebral artery as it exits the sylvian fissure, (2) branches of superior ramifications of the MCA, and (3) inferior loops of the MCA.
151.D. MAOA and MAOB are associated with the outer mitochondrial membrane.
152.A. The metencephalon is a secondary vesicle that becomes the pons, cerebellum, and upper part of the fourth ventricle. The myelencephalon becomes the medulla and the lower part of the fourth ventricle.
153.A. The tectorial membrane is a projection of the spiral limbus that overlies hair cells of the organ of Corti. The basilar membrane supports the organ of Corti and separates the cochlear duct from the scala tympani. The vestibular (Reissner’s membrane) separates the scala vestibuli from the cochlear duct.
154.B. Solitary projections to the nucleus ambiguus are largely bilateral and are the intermediate neurons in the pathway for the gag reflex.
155.C. The film shows a grade I spondylolisthesis at L4–L5. Although management of this problem is wide ranging, from the choices given the best management is a pedicle screw fusion at the concerning levels (L4–L5).
156.B. The GABA-B receptor is activated by the GABA analogue baclofen, is not chloride dependent, and is bicuculline insensitive. GABA-C is found in the retina, hippocampus, and cerebellum, and is insensitive to baclofen and bicuculline.
157.C. Structures that pass above the tendinous ring are the lacrimal nerve, frontal nerve, and CN IV (trochlear).
158.C. The most common causative organism of brain abscesses in trauma is Staphylococcus.
159.B. The most common causative organism of brain abscesses in adults due to chronic otitis is Streptococcus.
160.A. The most common causative organisms of brain abscesses in neonates are Citrobacter, Bacteroides, Proteus and gram-negative bacilli.
161.A. Tranylcypromine is an inhibitor of MAOA. Deprenyl is a specific inhibitor of MAOB.
162.B. The floor plate contains the ventral white commissure.
163.E. Sturge–Weber syndrome occurs sporadically without Mendelian inheritance and is of unknown etiology.
164.E. There are nonchoroid plexus sites of cerebrospinal fluid (CSF) production. Likewise there are sites of absorption other than the arachnoid granulations (paranasal sinuses, cervical lymphatics, exiting nerve roots, and transependymal flow).
165.C. In patients with known systemic cancer, 10–15% of single brain lesions are cerebral abscesses or primary brain tumors.
166.A. Vigabatrin interferes with GABA breakdown, whereas tiagabine interferes with GABA reuptake.
167.B.
168.B. Lesions placed too laterally during thalamotomy risk injury to the internal capsule (posterior limb). Lesions placed too posterior may cause contralateral hemisensory deficits owing to injury of the ventralis caudalis (VC) nucleus.
169.B. Cyclosporine along with some of the newer immunosuppressive agents (FK-506 or tacrolimus) work at the level of the T cells by inhibiting expression of IL-2.
170.E. The perforating arteries from the Pcom are termed the anterior thalamo-perforating arteries. Those from the P1 are called the posterior thalamo-perforating arteries. Those from P2 are termed the thalamo-geniculate arteries.
171.D.
172.E. The basal plate gives rise to the hypoglossal nucleus, nucleus ambiguus, dorsal motor nucleus of the vagal nerve, and inferior salivatory nucleus.
173.B.
174.B. Kocher’s point places the catheter in the frontal horn of the lateral ventricle. One can measure 1 cm anteriorly to the coronal suture or 3.5 cm in front of the bregma. This precaution is to avoid the motor strip. Keen’s point would be used for placement of the catheter in the trigone and would require entrance through the posterior parietal region.
175.B. The MRI demonstrates absent flow voids in the left vertebral artery, a finding seen in Wallenberg syndrome.
176.C. Clonazepam acts by increasing GABA-A opening frequency and does not have any hepatic enzyme–inducing properties.
177.A.
178.E. Freezing episodes and postural instability do not appear to be improved with pallidotomy.
179.C. Neurological involvement in HIV infection is more common in children than in adults. Neurological complications occur in > 40% of patients with HIV infection. They are the presenting feature of AIDS in 10–20% of patients. The prevalence of neuropathological abnormalities upon autopsy is 80%. Although an ongoing decline in HIV-associated CNS disease has been seen in very recent years, the mortality from these diseases remains elevated.
180.C.
181.B. Serotonin is found in many cells that are not neurons, such as platelets, mast cells, and enterochromaffin cells. In fact, the brain accounts for only about 1% of body stores of serotonin.
182.E. The alar plate gives rise to the layers of the superior colliculus and to the nuclei of the inferior colliculus.
183.A. Studies comparing nucleus pulposus material from disk herniation versus painful degenerative disk disease have shown that protein expression of tumor necrosis factor-α (TNF-α) and interleukin (IL)-8 is increased in the degenerative disk disease group, and both groups had similar levels of IL-1β, IL-6, and IL-12. Therefore, TNF-α and IL-8 may be promising candidates to treat patients with diskogenic back pain on a molecular level.
184.D. When dissecting below the arcuate line, the transversalis fascia is the only fascial layer between the rectus abdominis and the peritoneum.
185.B. Cranial neuropathies are a more common presenting sign of ependymomas than other tumors due to their tendency to arise from the floor of the fourth ventricle. Medulloblastomas typically arise from the inferior medullary velum.
186.D. Lissauer’s tract caps the dorsal horns, and these fibers terminate in the substantia gelatinosa (lamina II).
187.B. The limen insula is part of the primary olfactory cortex and is found at the junction of the insular and frontal lobe cortex.
188.C. If the electrode is correctly placed, visual thresholds are usually between 2 and 3 V. Higher values indicate that the electrode is too far superior. Lower values indicate that the electrode is too far inferior.
189.C.
190.B.
191.B
192.A. In stiff person syndrome, the stiffness primarily affects the truncal muscles and is superimposed by spasms, resulting in postural deformities. Chronic pain, impaired mobility, and lumbar hyperlordosis are common symptoms. The pattern of inheritance is unknown. Patients generally have high amounts of glutamic acid decarboxylase antibody titers.
193.B. Inflammatory mediators including interleukin (IL)-1β, IL-6, IL-8, and tumor necrosis factor-α are expressed at higher levels in “diseased” intervertebral disks.
194.E.
195.A.
196.D. Enlarged pituitary stalk may be due to sarcoidosis, which can present with elevated angiotensin-converting enzyme levels. It may also be due to Langerhans cell histiocytosis, which may present with eosinophilic granuloma. It can occur in cases of meningitis in children. It is very rarely associated with primary pituitary tumors.
197.D. Central facial palsy is usually characterized by either hemiparalysis or hemiparesis of the contra-lateral muscles in facial expression. Muscles on the forehead are typically intact. Patients have lost voluntary control of muscle movement in the face; however, muscles in the face involved in spontaneous emotional expression usually remain intact.
198.C.
199.A. Esthesioneuroblastoma has a variable outcome that is primarily prognosticated by the extent of involvement at presentation (Kadish stage and lymph nodes metastasis) and completeness of resection.
200.E. Brainstem auditory evoked potentials (BSAEP) measure the timing of electrical waves from the brainstem in response to clicks or tone bursts in the ear. Computer averaging over time filters background noise to generate an averaged response of the auditory pathway to an auditory stimulus. Three waves (I, III and V) are plotted for each ear. The waveform represents specific anatomical points along the auditory neural pathway: the cochlear nerve and nuclei (waves I and II), superior olivary nucleus (wave III), lateral lemniscus (wave IV), and inferior colliculi (wave V). The most reliable indicator of retraction during vestibular schwannoma surgery from the BSAEP is the interaural latency differences in wave V; the latency in the abnormal ear is prolonged.
201.B.
202.E. Golgi tendon organs are sensitive to muscle tension.
203.D. Lyme disease is an inflammatory disease caused by the spirochetes Borrelia burgdorferi, which are transmitted by the bite of infected Ixodes ticks. Lyme disease is endemic in Massachusetts, Connecticut, Maine, New Hampshire, Rhode Island, New York, New Jersey, Pennsylvania, Delaware, Maryland, Michigan, and Wisconsin. It is categorized into early localized, early disseminated, and late. There may be an erythema migrans or systemic complaints in the early localized phase. Early disseminated Lyme disease can present with many central nervous system manifestations, including meningitis, altered mental status, radiculopathy and cranial neuropathy. If left untreated, sequelae include rheumatologic symptoms (monoarticular or oligoarticular arthritis) in 60%, neurologic signs and symptoms in 10%, and cardiac complications in 5% of cases.
204.A. Shunt nephritis is a well-described complication of ventriculoatrial (VA) shunts. VA shunt complications are much more severe and potentially life-threatening than ventriculoperitoneal (VP) shunt complications.
205.C. There is a paucity of mitoses and no necrosis in dysembryoplastic neuroepithelial tumors (DNET).
206.D. The patient likely presents with an adrenocorticotropic hormone (ACTH)-secreting macroadenoma. Proper evaluation prior to surgery includes ophthalmologic and endocrine consultations and an endocrine panel of laboratory tests.
207.D.
208.D. All of the information that is passed between the brainstem and the cerebellum enters and exits through one of three cerebellar peduncles: (1) inferior cerebellar peduncle or restiform body at the level of the medulla, (2) middle cerebellar peduncle or brachium pontis at the level of the pons, (3) superior cerebellar peduncle or brachium conjunctivum at the level of the midbrain. The vestibulocerebellar tract traverses the juxtarestiform body.
209.C. Higher levels of TrkA are seen in neuroblastomas with favorable histology. The other factors listed are associated with a worse prognosis in neuroblastomas.
210.C.
211.C. Choline acetyltransferase is the definitive marker for cholinergic neurons. Hemicholimium-3 blocks the high-affinity cholinergic reuptake process.
212.A. Tanycytes are a variety of ependymal cells found in the wall of the third ventricle. The tanycyte is a cell with intermediate features between astrocytes and ependymal cells.
213.B.
214.D.
215.E.
216.C. The diagram shown represents the lumbar plexus, structure A is the ilioinguinal nerve, B is the genitofemoral nerve, C is the lateral femoral cutaneous nerve, D is the femoral nerve, and E is the obturator nerve.
217.B.
218.B. Facial agnosia (prosoprognosia) results from bilateral damage to the medial basal occipitotemporal cortex.
219.E. All of the above may be the presentation in children with neuroblastomas. Diarrhea is from vasoactive intestinal polypeptide (VIP) secretion by the tumor. Ondine’s curse results from impaired autonomic control of respiration.
220.C.
221.D. The synthesis of NO (nitrous oxide) involves the conversion of L-arginine into NO and citrulline. All three isoforms of nitric oxide synthase (NOS) require tetrahydrobiopterin as a cofactor and NADPH as a coenzyme.
222.B. The substantia gelatinosa (Rexed lamina II) is found at all cord levels and is homologous to the spinal trigeminal tract. It is associated with light touch, pain, and temperature sensation, and it integrates input for the ventral and lateral spinothalamic tracts.
223.A. Vein of Galen malformation may be defined as a direct arteriovenous (AV) fistula between choroidal and/or quadrigeminal arteries and an overlying single median venous sac; it is rare, representing only < 1% of all intracranial arteriovenous malformations (AVMs). Neonatal patients present with an abrupt onset of high-output cardiac failure; as much as 80% of the cardiac output may pass through the fistula. An audible bruit may be present. Another type of vein of Galen malformation (VOGM) (presenting with ocular symptoms and developmental delay) is typically thalamic or midbrain with deep drainage to the vein of Galen (VOG).
224.D. The scan demonstrates an intramedullary cavernoma. These lesions tend to bleed in patients of young age, show a clear sensory level, present with subarachnoid hemorrhage or by progressive ascending paraplegic syndrome. The definitive therapy is microsurgical elimination.
225.B. The arcuate eminence is a prominence on the anterior surface of the petrous portion of the temporal bone corresponding to the position of the superior semicircular canal.
226.D.
227.B. The calamus scriptorius is an anatomic structure along the inferior part of the rhomboid fossa; the narrow lower end of the fourth ventricle between the two clavae.
228.D. Delta waves occur with deep sleep, infancy, and brain disease.
229.E. The stylohyoid is innervated by VII. The styloglossus is innervated by XII. The stylopharyngeus is innervated by IX.
230.A. The sagittal vertical axis is the distance between the C7 plumb line and the posterosuperior corner of S1 in the sagittal plane.
231.A. Allodynia is a condition in which a painful response is produced by an innocuous mechanical stimulation. It is the result of sensitization of spinothalamic neurons in the dorsal horn and the failure of descending systems to control the activity of these neurons. Alloesthesia is characterized by a painful stimulus on one side of the body that is thought to be on the other side.
232.D. Clarke’s nucleus is found at the base of the dorsal horn and corresponds to Rexed VII lamina. Clarke’s column extends from C8 or T1 to about L3. Clarke’s nucleus is homologous to the accessory cuneate nucleus of the medulla. It subserves unconscious proprioception from the muscle spindles and Golgi tendon organs and is the origin of the dorsal spinocerebellar tract.
233.E. Basal encephaloceles should be treated as early as possible. Children with basal encephaloceles in the nasopharynx are at significant risk of developing meningitis.
234.B. The anterior limb of the internal capsule (on horizontal section) can be found between the caudate nucleus and the corpus striatum (globus pallidus and putamen). Clinically important tracts lie in the genu and posterior limb. The posterior limb (on horizontal section) can be found between the thalamus and the corpus striatum (globus pallidus and putamen). The posterior limb of the internal capsule contains corticospinal fibers.
235.D.
236.A.
237.B.
238.C.
239.D. The greater occipital nerve is a sensory nerve from the dorsal ramus of C2.
240.C. Thromboxane synthesis inhibitors lead to a buildup of arachidonic acid.
241.C. The lateral portion of the substantia nigra pars reticulata (SNpr) is connected with cortical and brainstem areas that control eye movements. SNpr is GABAergic and inhibitory to the VLm (medial part of the ventrolateral thalamus) and VAmc (magnocellular part of the ventral anterior thalamus).
242.A. The dorsal lateral sulcus receives the dorsal roots.
243.D. The scan shows a diffusely enhancing brainstem glioma. Biopsy is usually not recommended in this case. Hyperfractionated radiation therapy has been shown to improve survival. Brainstem gliomas represent 10–20% of childhood CNS tumors. There are currently no proven chemotherapeutic regimens.
244.B. Pelvic incidence: the angle between the perpendicular to the sacral plate at its midpoint and the line connecting this point to the middle axis of the femoral heads. It is an anatomical parameter, unique to each individual, independent of the spatial orientation of the pelvis. Sacral slope: the angle between the superior plate of S1 and a horizontal line. Pelvic tilt: the angle between the line connecting the midpoint of the sacral plate to the axis of the femoral heads, and the vertical.
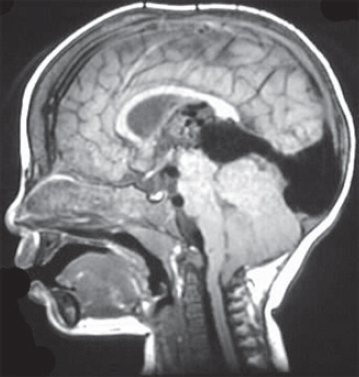
245.E. The MRI represents a midsagittal section demonstrating a large sellar and suprasellar mass that is compressing the optic chiasm. Slightly elevated prolactin level may be secondary to the stalk effect.
246.E.
247.D.
248.B. Lhermitte–Duclos disease is an uncommon cerebellar dysplasia that is characterized by hypertrophy of granular-cell neurons, and axonal hypermyelination in the molecular layer. Also known as dysplastic gangliocytoma of the cerebellum, it may occur in the setting of Cowden disease caused by a PTEN germline mutation.
249.A. There is no sensory deficit and no decrease in corneal reflex. There are no other symptoms in the other cranial nerves.
250.B. The liquid embolic agent n-butyl cyanoacrylate is used in interventional neuroradiology. The embolic agents that are particulate in nature include polyvinyl alcohol, platinum coils, and silk thread.
251.C. The Glasgow Coma Scale score (GCS score) in this case would be 13. Eyes open to speech (3), the patient is confused (4), and he obeys motor commands (6)
252.B. The ciliospinal center of Budge is found in the lateral horn at T1. This is a sympathetic nucleus that innervates the radial muscle of the iris (dilator pupillae) and the nonstriated superior and inferior (Müller) muscles.
253.E. Aspirin decreases all anticonvulsant levels.
254.A. Posterior inferior cerebellar artery (PICA) syndrome causes decreased contralateral pain and temperature of the body.
255.C. Teardrop fractures occur when a fracture occurs on the anteroinferior edge of the vertebral body. The injury is due to hyperflexion and is unstable. Teardrop fractures are associated with anterior cord syndrome.
256.B.
257.B. Dura and blood vessels are formed from mesoderm.
258.C. The most common primary septal tumor is astrocytoma.
259.C. The superior cerebellar artery is the most commonly conflicting artery in trigeminal neuralgia.
260.A. The ELANA technique (excimer laser-assisted nonocclusive anastomosis) may be used to anastomose arteries.
261.B. This MRI scan demonstrates a unilateral jumped facet with rotation in the cervical cord, compromising the spinal canal.
262.D. This particular AVM is best-graded 4A. Its medium size (2), eloquent location (1), and deep drainage (1) place it as a Spetzler–Martin grade 4. The fact that it has stenotic venous drainage gives it a subclassification of 4A.
263.B. Biot (irregular breathing) is caused by a lesion in the dorsomedial medulla.
264.B. The anterior choroidal artery supplies the internal globus pallidus, posterior limb of the internal capsule, and temporal horn of the choroid plexus.
265.D. Pronator teres syndrome is different from carpal tunnel syndrome in that patients with pronator teres syndrome exhibit numbness in the palm, and nocturnal exacerbations are rare.
266.C. The MRI scan represents a brain midsagittal section demonstrating descent of the cerebellar vermis or tonsils consistent with a Chiari malformation, given the age of the patient and the absence of other findings (e.g., hydrocephalus or medullary kinking), this most likely represents a Chiari type 1 malformation.
267.C.
268.B.
269.B. Although it is true that the pain starts at V2 (the lower side of the nose) and then involves V3 and V1, it is only necessary to treat the trigger zone.
270.E. Gerstmann’s syndrome is caused by a dominant parietal lobe lesion (angular gyrus) and includes agraphia without alexia (patient can read but cannot write). Astereognosis is also caused by dominant parietal lobe lesions but is not part of Gerstmann’s syndrome.
271.E. Epidermoids of the skull show a lytic defect with a scalloped, sclerotic rim. They are slow growing and rarely show malignant transformation.
272.E.
273.B. Nightmares occur during REM sleep; night terrors may occur in either stage 3 or 4 sleep. Stage 4 sleep is associated with delta waves.
274.A.
275.D.
276.B. A high-riding jugular bulb may be encountered during the drilling portion and should be tamponaded with hemostatic products and cottonoids.
277.B. The subcommissural organ is the only circumventricular organ with an intact blood–brain barrier (BBB).
278.B. Dysgeusias are particularly prevalent in the elderly and are often associated with the use of antihypertensives (e.g., captopril).
279.C. Gamma knife treatment is the best mode of therapy for an AVM that is smaller than 3 cm and located in an eloquent area. The angiogram shows a small subcortical right parietal arteriovenous malformation with filling vessel arising from a branch of the right middle cerebral artery. Venous drainage is noted into the upper sagittal sinus.
280.D. Foster–Kennedy syndrome is usually caused by an olfactory groove or medial-third sphenoid wing tumor (usually meningioma). The classic triad is anosmia (ipsilateral), central scotoma (ipsilateral), and papilledema (contralateral).
281.B. Pick’s disease is characterized by severe focal atrophy commonly in the frontal and temporal lobes. This results in mental status and personality changes occurring in Pick’s patients. Pick bodies are positive for tau protein.
282.B. Fibrillation potentials are triphasic and last 1–5 ms caused by the activity of one fiber.
283.B. Sleep spindles (the burst described) and K complexes (sharp slow waves of high amplitude) are characteristic of stage 2 sleep.
284.D. The bony promontory seen in the picture is the posterior clinoid process and may be drilled carefully to expose the neck of the aneurysm.
285.D. The suprascapular nerve is trapped in the suprascapular notch. This nerve is the branch of the superior trunk. Atrophy of the supraspinatus and infraspinatus can result.
286.C. The abducens nerve crosses the medial lemniscus on exiting the brainstem.
287.B. The correct units are 50 mL/100 g/min.
288.D.
289.A. Removal of frontal meningiomas may improve attentional functions. There are minimal differences in memory, visuoconstructive abilities, or executive functions.
290.E. The secretion of prolactin by lactotroph cells is inhibited by dopamine released by hypothalamic neurons.
291.C. The substantia nigra pars reticulata neurons related to saccadic eye movements decrease their activity during the saccade.
292.D.
293.A. Research with model systems of seemingly disparate species (i.e., marine snail and albino rat) suggest that neural mechanisms involved in associative learning may be highly conserved across species.
294.E.
295.C. Hypothermia is characterized by J-point elevation.
296.A. Anterior encephaloceles are compatible with normal intelligence in the majority of patients. Atretic encephaloceles also appear not to influence intellectual development and also have a low incidence of hydrocephalus.
297.A. Giant cell glioblastoma is shown in the slide. The hallmark of giant cell glioblastoma is predominance on multinucleated giant cells and a high frequency of the TP53 mutation.
298.D. These features should not necessarily prompt the diagnosis of glioblastoma.
299.B. The supramarginal gyrus is at the posterior reach of the sylvian fissure.
300.A. Avellis’s syndrome is caused by a brainstem lesion that limits vagal innervation unilaterally, resulting in ipsilateral paralysis of the vocal cord and soft palate and loss of sensitivity to pain and temperature in the contralateral leg, trunk, arm, and neck. This syndrome is also called ambiguospinothalamic paralysis.
301.E. Bicuculline is a GABA-A antagonist. Muscimol is a GABA-A agonist. Kynurenate is a glutamate antagonist. Picrotoxin is a GABA inhibitor.
302.B. There is increased production of PMP22 in Charcot–Marie–Tooth disease.
303.C. Neurons in the spinal nucleus and in the ventral parts of the chief sensory nucleus give rise to the crossed ventral trigeminothalamic tract.
304.D. In stroboscopic illumination at flicker rates below 15 Hz, the motion system is disabled. This explains why nightclub dancers are seen as moving discontinuously under a strobe light.
305.C. The tectospinal tract decussates in the dorsal tegmental decussation. Tectospinal fibers originate from deeper layers of the superior colliculus and distribute to cervical cord levels. Rubrospinal fibers decussate in the ventral tegmental decussation.
306.A. In the Royal Melbourne Hospital series of paranasal sinus involvement treated by craniofacial resection, sphenoid sinus involvement was the major predictor of later tumor recurrence.
307.E. Bipolar cells serve as interneurons between photoreceptor cells and ganglion cells.
308.D.
309.B.
310.C. The connatal form (type II) is clinically more severe and symptoms begin in the neonatal period. Pelizaeus–Merzbacher disease (PMD) results from mutations affecting the gene for proteolipid protein (PLP).
311.D. The pontocerebellar tract passes to the cerebellum via the middle cerebellar peduncle. The ventral spinocerebellar tract and the tectocerebellar tract pass through the superior cerebellar peduncle.
312.C. The lateral zone (dentate) sends fibers to the VL thalamus and motor cortex (area 4). A lesion of the anterior lobe may cause slight hyperreflexia.
313.A. Dendrodendritic synapses have been found in the olfactory bulb and have been shown to be inhibitory; the granule cells processes make synaptic contacts with dendrites of mitral cells. Axodendritic synapses are excitatory. Axosomatic synapses are inhibitory, and a classic example is the cerebellar basket cell contacting the Purkinje cell.
314.B. The parvocellular system of the dorsal lateral geniculate nucleus makes up about 80% of the total ganglion cell number.
315.E. During a neurosurgical procedure, a sudden decrease in end tidal CO2 suggests venous air embolus and may even precede the appreciation of changes by the precordial Doppler.
316.E. These structures run in the floor of the body of the lateral ventricle.
317.A. The contents of the cubital fossa from medial to lateral are the median nerve, brachial artery, biceps brachii tendon, and radial nerve.
318.D. The teres minor rotates the arm laterally.
319.C. The internal cerebral vein position can be confirmed by superimposing the angiogram of the medial posterior choroidal artery with the venous phase. The internal cerebral vein and the medial posterior choroidal artery occupy the same position when the arterial and venous phase are superimposed. Both of these structures course within the cistern of the velum interpositum.
320.B.
321.D. The Botzinger complex is the principle source of reciprocal inhibition in the respiratory network. It comprises a cluster of cells at the rostral-most tip of the ventral respiratory group.
322.D. The posterior cord gives rise to the upper subscapular, lower subscapular, and thoracodorsal nerves. The latissimus dorsi is innervated by the thoracodorsal nerve. The subscapularis muscle is innervated by the upper and lower subscapular nerve. The teres major is innervated by the lower subscapular nerve.
323.A. The vast majority of children present with ischemic symptoms (transient ischemic attacks (TIAs), extremity weakness), whereas adults typically present with hemorrhage.
324.C. Valproic acid has a short half-life (~ 8 hours). Association with platelet dysfunction should alert the surgeon to the possibility of bleeding problems, especially in epilepsy cases.
325.B. Isoflurane allows patients to emerge from anesthesia faster, and there is less hepatic effect from this agent. In addition, isoflurane produces the least increase in cerebral blood flow (CBF) of inhalational anesthetics.
326.C. The glomus is a prominent tuft of choroid plexus found in the atrium.
327.C. The axillary nerve passes posteriorly around the surgical neck of the humerus. The radial nerve lies in the radial groove of the middle of the shaft of the humerus. The ulnar nerve passes behind the medial epicondyle. All three of these nerves are susceptible to humerus fractures since they lie in close contact with bone.
328.C. The premotor area plays a role in programming and sequencing learned complex movements.
329.E.
330.A. Theta activity has a frequency of 4–7 Hz. Other common electroencephalographic (EEG) rhythms are delta (0–3 Hz), alpha (8–13 Hz), and beta (> 13 Hz).
331.B. The mesencephalic nucleus of the trigeminal nerve has pseudounipolar neurons. The mesencephalic nucleus extends from the pons to the upper midbrain. It receives input from muscle spindles and pressure receptors.
332.B. These second-order neurons will give rise to axons that enter the cerebellum via the superior cerebellar peduncle. The ventral spinocerebellar tract conveys efference copies of motor commands for the lower extremities.
333.B. Chromophobic cells lack cytoplasmic granules. They represent acidophil or basophil cells after the release of hormone-containing granules. They have no stain reaction after PAS stain.
334.D. The extent of mesiobasal resection determines the outcome after temporal lobectomy for intractable complex partial seizures.
335.E. Sydenham’s chorea is the most common type of chorea. Also known as St. Vitus’s dance, this chorea occurs mainly in young females after a bout of rheumatic fever.
336.D. This is decadron. A postoperative course of an H2-receptor blocker is indicated for patients on glucocorticoid treatment.
337.D.
338.B. Ventralis intermedius (Vim) stimulation is the procedure of choice when contralateral thalamotomy has been performed or is anticipated.
339.C. Temozolomide (TMZ) is an orally administered chemotherapeutic (alkylating) agent with minimal side effects that readily crosses the blood–brain barrier and is approved for treating anaplastic astrocytomas.