Atlas of Pathologic Substrates of Epilepsy
Richard A. Prayson
Ajay Gupta
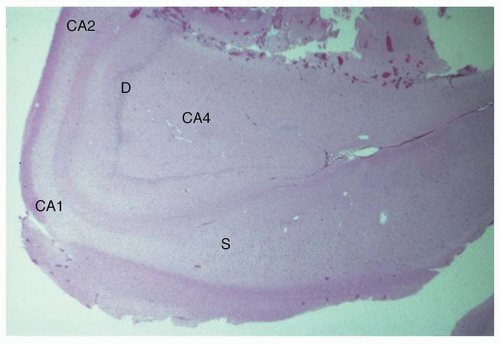 Figure 1.1 Low-magnification appearance of hippocampus in a patient with hippocampal sclerosis (HS). An adult patient who underwent anterior temporal lobectomy for treatment of intractable temporal lobe epilepsy. HS is the most common cause of intractable partial epilepsy in adults. The disorder is generally marked by preferential loss of neurons in the dentate (D), CA4 region, CA1 region, and subiculum (S). A lesser degree of neuronal loss may be observed in the CA3 and CA2 regions. Loss of neurons is accompanied by gliosis and, in severe cases, by grossly evident atrophy. |
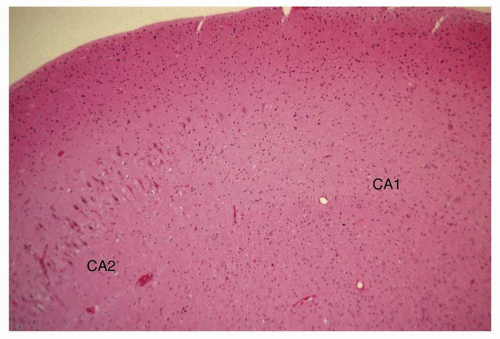 Figure 1.2 Higher-magnification appearance of the hippocampus in hippocampal sclerosis (HS) at the interface between the CA2 and CA1 regions. There is a marked loss of neurons in the CA1 region with gliosis. |
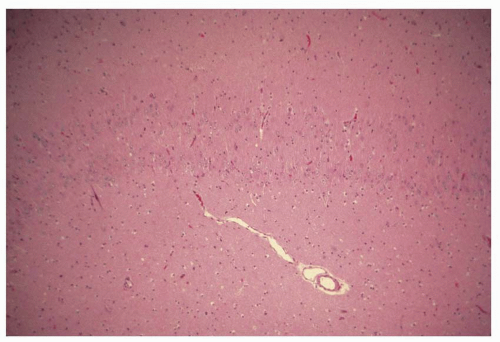 Figure 1.3 Histologic appearance of double dentate, marked by two bands of neurons in the hippocampus. This represents a form of hippocampal dysplasia, an infrequent cause of temporal lobe epilepsy that may be seen as a dysmorphic hippocampal formation on high-definition, three-dimensional, volume acquisition sequences on brain magnetic resonance imaging (MRI). |
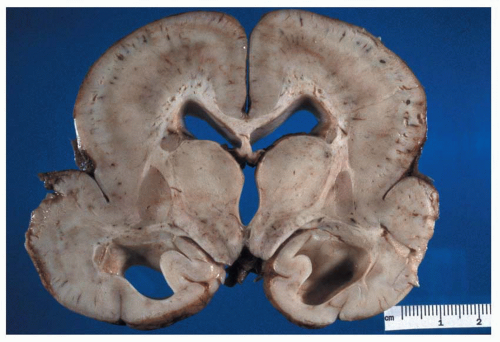 Figure 1.4 The gross appearance of lissencephaly (agyria), characterized by a lack of gyral formation and a decreased number of sulci. Note the enlargement of the ventricles, suggesting parenchymal volume loss. The cortex is usually thickened on cross section. Microscopically, an abnormally layered cortex is seen, typically three to five layers. Children with lissencephaly usually present with epileptic spasms, severe global developmental delay, microcephaly, and marked hypotonia during early infancy. |
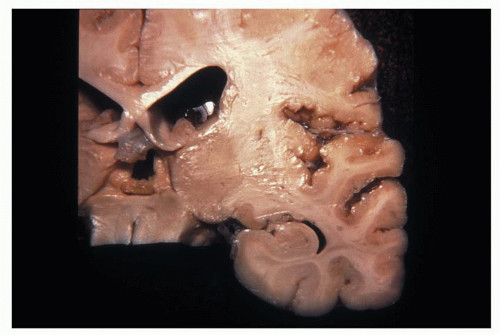 Figure 1.5 Gross appearance of perisylvian polymicrogyria (micropolygyria), marked by the focal presence of small, irregular gyri separated by shallow sulci. The cortex is often thinned and microscopically consists of two to four layers. The leptomeninges overlying polymicrogyria may be abnormally hypervascular because of a persistence of fetal leptomeningeal vascularization. (Photograph courtesy of Dr. Bette Kleinschmidt-DeMasters.) C congenital bilateral perisylvian polymicrogyria (CBPP) usually presents with seizures during childhood. Other clinical findings in patients with CBPP include pseudobulbar paresis, dysarthria, swallowing difficulties, and tongue paresis accompanied by the inability to protrude the tongue and perform lateral tongue movements. |
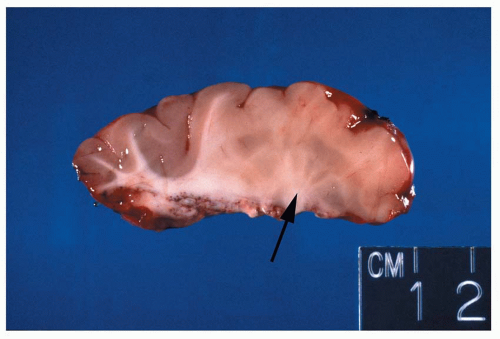 Figure 1.6 Gross appearance of cortical dysplasia, marked by an indistinct gray/white interface (right portion of cross section [arrow]) with evidence of gray matter tissue abnormally placed in the white matter (nodular heterotopia). Most of the focal cortical dysplasias are sporadic congenital malformations and, as a group, are an important cause of intractable epilepsy that is surgically remediable. |
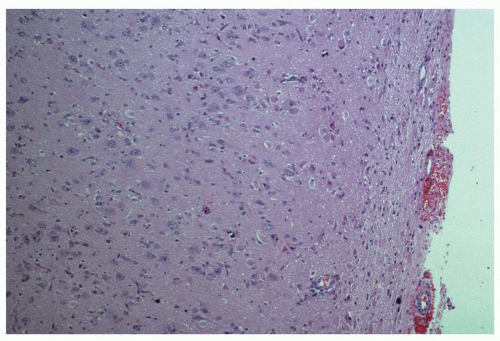 Figure 1.7 Histologic appearance of cortical dysplasia, marked by a loss of normal cortical lamination, increased cellularity, and malpositioning of neurons within the cortex. Neurons normally have their apical dendrites oriented perpendicular with respect to the surface of the brain. |
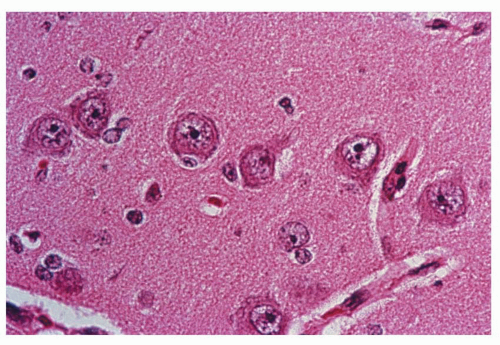 Figure 1.8 High-magnification appearance of neurons in cortical layer two of the parietal lobe in a patient with cortical dysplasia. The neurons are abnormally enlarged in size (neuronal cytomegaly), with no further evidence of dysmorphic features. |
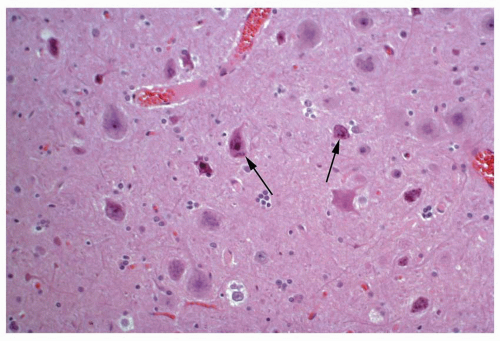 Figure 1.9 Histologic appearance of neurons in cortical layer three of the temporal lobe in a patient with cortical dysplasia. The neurons are marked by an abnormal cytologic appearance (dysmorphic neurons) (arrows), including abnormal nuclear morphology and atypical distribution of Nissl substance. In addition, neurons are haphazardly arranged within the cortex. |
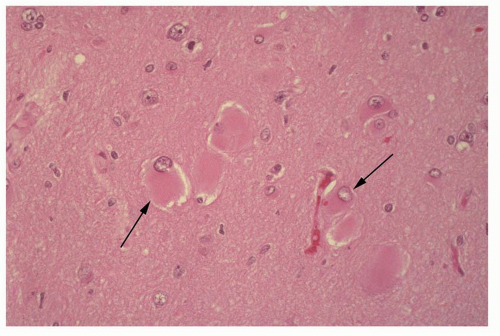 Figure 1.10 Histologic appearance of balloon cells (arrows) in the setting of cortical dysplasia. Balloon cells are marked histologically by the presence of abundant eosinophilic cytoplasm and eccentrically placed nuclei. Multinucleation may be observed. The derivation of these cells is still debated. A subset of balloon cells stain with markers of both glial differentiation (glial fibrillary acidic protein) and neural differentiation (neuron-specific enolase). |
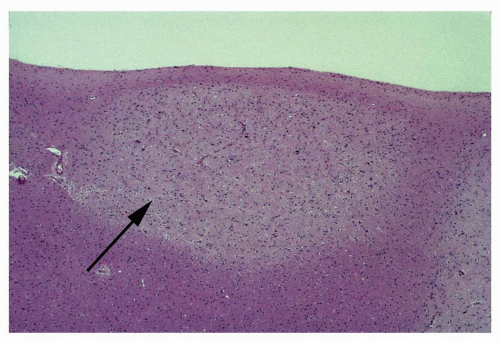 Figure 1.11 Microscopic appearance of a subependymal nodular heterotopia of gray matter (arrow). Microscopically, the nodule is marked by a mixture of neural and glial cells arranged in a disorganized fashion. Heterotopias are collections of mostly normal-appearing neurons in an abnormal location, presumably as a result of a disturbance in migration. |
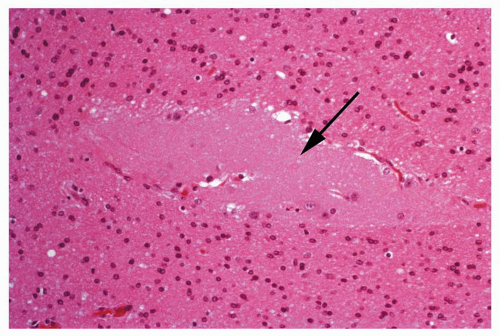 Figure 1.12 Small focus of heterotopic gray matter situated in the deep white matter of the frontal lobe region (arrow).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|



