5 Blink Reflex
Anatomy
The afferent limb of the blink reflex is mediated by sensory fibers of the supraorbital branch of the ophthalmic division of the trigeminal nerve (cranial nerve V1) and the efferent limb by motor fibers of the facial nerve (cranial nerve VII). Just as with the corneal reflex, ipsilateral electrical stimulation of the supraorbital branch of the trigeminal nerve elicits a facial nerve (eye blink) response bilaterally. Stimulation of the ipsilateral supraorbital nerve results in an afferent volley along the trigeminal nerve to both the main sensory nucleus of V (mid-pons) and the nucleus of the spinal tract of V (lower pons and medulla) in the brainstem. Through a series of interneurons in the pons and lateral medulla, the nerve impulse next reaches the ipsilateral and contralateral facial nuclei, from which the efferent signal travels along the facial nerve bilaterally (Figure 5–1).
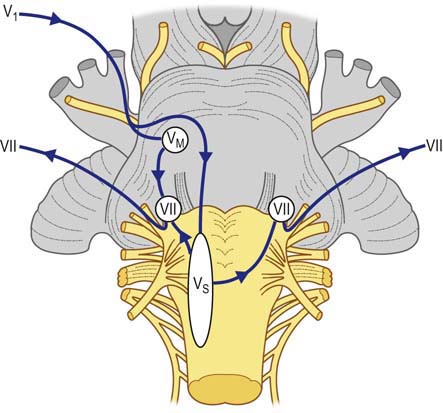
FIGURE 5–1 Blink reflex anatomy.
(Modified from Chusid JC. Correlative neuroanatomy and functional neurology, 18th ed. Stamford, CT: Appleton & Lange, 1982, with permission.)
Blink Reflex Procedure
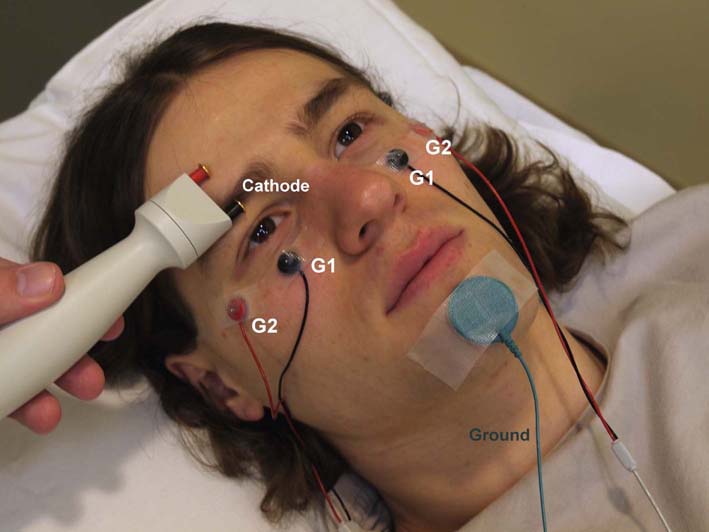
The patient should be in a relaxed state, lying supine on the examining table, with the eyes either open or gently closed (Box 5–1). Recording is performed simultaneously from both sides of the face using a two-channel recording apparatus. Surface recording electrodes are placed over the inferior orbicularis oculi muscles bilaterally (Figure 5–2). For recording the compound motor action potential from the orbicularis oculi muscle, the active recording electrode (G1) is best placed below the eye just lateral and inferior to the pupil at mid-position. The corresponding reference electrodes (G2) are placed just lateral to the lateral canthus bilaterally. Alternatively, recording can be done with small concentric needle electrodes placed in the orbicularis oculi bilaterally. The ground electrode is placed on the mid-forehead or chin.
Box 5–1
Blink Response Procedure
1. The patient should be in a relaxed state, lying supine on the examining table, with the eyes either open or gently closed.
2. Recording from both orbicularis oculi muscles is performed simultaneously.
3. Active recording electrodes are placed below the eye just lateral and inferior to the pupil at mid-position, with the reference electrodes placed just lateral to the lateral canthus.
4. A ground electrode is placed over the mid-forehead or chin.
5. Sweep speed set at 5 or 10 ms/division.
6. Sensitivity set at 100 or 200 µV/division.
7. Motor filter settings are 10 Hz and 10 kHz.
8. Stimulate each supraorbital nerve (preferably with pediatric prong stimulator) over medial eyebrow, recording orbicularis oculi bilaterally. Allow several seconds between successive stimulations to prevent habituation.
9. For each side, 4–6 stimuli are obtained on a rastered tracing and superimposed to determine the shortest response latencies.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


