Brief Review of the Anatomy of the Head, Spine, Brain, and Spinal Cord
Juan C. Troncoso
The first goal of this chapter is to reacquaint the reader with the gross anatomy and landmarks of the skull, spine, brain, and spinal cord to facilitate an accurate description of lesions. The second goal is to provide a succinct review of the clinical manifestations associated with lesions of specific regions of the brain and spinal cord.
SCALP
The scalp is the cover of the skull and consists of several layers, including the external skin and hair, subcutaneous tissue, the galea or epicranial aponeurosis, and the periosteum (Fig. 2.1). The galea provides attachment to the occipitalis and frontalis muscles. Over the squamous portion of the temporal bone, the temporalis muscle is inserted between the periosteum and the subcutaneous tissue. The subcutaneous tissue of the scalp is richly vascularized and can bleed profusely. The space between the galea and the periosteum constitutes a cleavage plane that allows the scalp to be stripped from the skull (i.e., to expose the skull for opening during autopsy). Blood can also dissect and enter into this space, giving origin to a subgaleal hematoma.
SKULL
The skull or cranium is the compartment that contains and protects the brain. The skull consists of an inferior platform or base of the skull and a dome, known as the calvaria or vault. The calvaria is marked by three major sutures (sagittal, coronal, and lambdoid) that are closed in the adult (Fig. 2.2A) but remain partially open in newborns and infants and form the anterior (bregma), posterior (lambda), and lateral fontanelles (Fig. 2.2B). The base of the skull is divided by the sphenoid and petrous ridges into three tiers denominated by the anterior, middle, and posterior fossae (Fig. 2.3). The inferior surface of the frontal lobes, also known as the orbitofrontal region, rests on the anterior fossa. The floor of the anterior fossa, which is also the roof of the orbit, is a thin lamina of bone that can fracture easily. For example, the floor of the anterior fossa may fracture as a result of the contrecoup impact of the brain in falls with occipital impacts (blow-out fracture).1 The temporal lobes lie on the middle fossa, and the cerebellum lies on the posterior fossa (the occipital lobes rest on the tentorium, as described below). At the center of the middle fossa lies the sella turcica, the seat of the pituitary gland. The surface of the anterior and middle cranial fossae is irregular, characterized by multiple bony ridges and small orifices through which blood vessels and nerves enter and exit the skull. The posterior fossa consists of an inclined central plane, known as the clivus, over which lies the brainstem and two lateral and posterior concave expansions that contain the cerebellar hemispheres. The foramen magnum is at the bottom of the posterior fossa, allowing the passage of the neuraxis and marking the transition of the medulla into the cervical cord. Unlike the anterior and middle cranial fossae, the surface of the posterior fossa is smooth. The same bones that form the base of the skull harbor multiple air-filled cavities known as sinuses. For example, the sphenoidal sinus is under the sella, and the frontal sinuses are under the anterior fossa. These sinuses, the frequent site of inflammation and infection, represent potential sources for infections to extend into the skull, meninges, and brain. This potential is greatly enhanced by fractures of the base of the skull. Notably, fractures of the base of the skull may result in communication between the
subarachnoid space and the paranasal sinuses or the nose. In this way, a fracture of the anterior fossa may result in a leak of cerebrospinal fluid through the nose.
subarachnoid space and the paranasal sinuses or the nose. In this way, a fracture of the anterior fossa may result in a leak of cerebrospinal fluid through the nose.
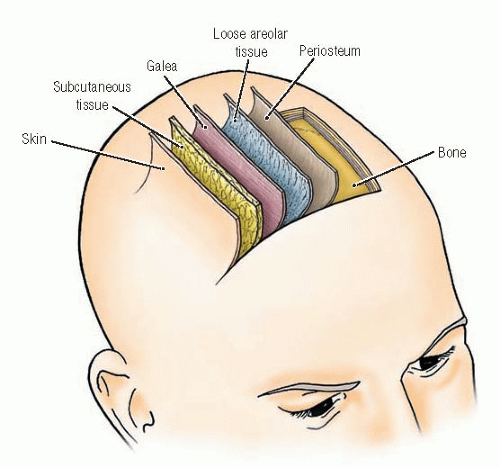 FIG. 2.1. Layers of soft tissues (scalp) covering the skull. (Adapted with permission from Agur AMR, Dalley AF. Grant’s Atlas of Anatomy. 12th Ed. Baltimore: Lippincott Williams & Wilkins, 2008:634.) |
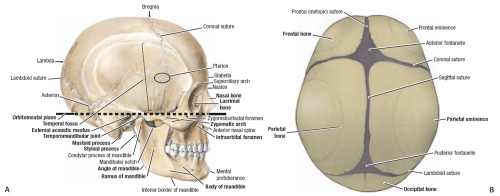 FIG. 2.2. A. Lateral view of skull. B. Superior view of skull in neonates or young infants. (Reprinted with permission from Agur AMR, Dalley AF. Grant’s Atlas of Anatomy. 12th Ed. Baltimore: Lippincott Williams & Wilkins, 2008:609, 612.) |
The calvaria are formed by the fusion of the frontal, parietal, temporal, and occipital bones. The bones of the calvaria are formed by two layers or tables of compact bone (diploe), with an intermediate layer of trabeculated bone, which contains a plexus of veins. The cranial dura mater is attached to the internal surface of the skull in such a way that fractures of the calvaria can lacerate the dura or dural vessels. The most common mechanism for the development of epidural hemorrhage is a fracture of the squamous portion of the temporal bone, with laceration of branches of the middle meningeal artery. The blood under pressure dissects the dura from the bone and forms a lens-shaped hematoma that compresses the brain.
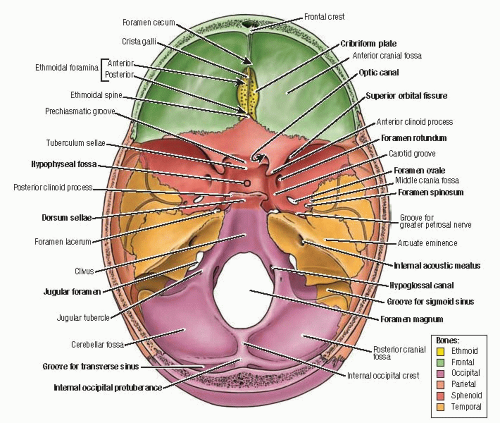 FIG. 2.3. Base of skull viewed from above. (Reprinted with permission from Agur AMR, Dalley AF. Grant’s Atlas of Anatomy. 12th ed. Baltimore: Lippincott Williams & Wilkins, 2008:619.) |
MENINGES
The brain and spinal cord are wrapped by three layers of connective tissue known collectively as meninges. These are the dura mater, arachnoid, and pia mater.
Dura Mater
The skull is lined internally with a tough layer of connective tissue designated the dura mater (e-Figs. 2.1 and 2.2). The dura mater has two major reflections: the falx, which runs vertically in the interhemispheric fissure, separating the cerebral hemispheres (Fig. 2.4A), and the tent of the cerebellum, which has an approximately horizontal orientation and separates the dorsal surface of the cerebellum from the inferior surface of the occipital lobes. A large opening, the tentorial notch, is present in the center of the tentorium for the passage of the brainstem (e-Fig. 2.2). Accumulations of blood or exudates may occur between the dura mater and the skull, known as epidural lesions, or between the dura mater and the brain, know as subdural lesions. Sometimes in newborns, intradural hemorrhages are noted within the two layers of the falx.
The dura mater also forms the walls of the venous sinuses that drain the brain into the jugular arteries. These sinuses include the superior (Fig. 2.4) and inferior sagittal, transverse, straight, and sigmoid sinuses. The cavernous sinus, which runs lateral to the sella, drains via the ophthalmic veins and pterygoid plexus into the veins of the face (e-Fig. 2.2).
Leptomeninges
The brain is covered by two delicate layers of connective tissue known as leptomeninges (Fig. 2.4). The pia mater, which is the most internal layer, adheres to the brain tissue and intimately follows the contour of the cortical mantle, thus covering from the crown of the gyri to the bottom of the sulci. Although delicate in appearance, the pia mater is an effective barrier that can prevent infectious agents and inflammatory exudates from extending directly from the subarachnoid space into the brain parenchyma. The arachnoid, placed between the pia and the dura mater, is also a thin and translucent membrane, like a cobweb, that covers the surface of the brain, bridging over the sulci of the cerebral cortex. The normal translucency of the arachnoid can be obscured by hemorrhage, exudates, or fibrosis. Between the pia and the arachnoid is the subarachnoid space. This space, which is continuous with the subarachnoid space surrounding the spinal cord, contains the cerebrospinal fluid, communicates with the ventricular system via the orifices of Luschka and Magendie (fourth ventricle), and projects into the brain parenchyma along perivascular sleeves known as Virchow-Robin spaces. The arachnoid has specialized structures—designated arachnoid granulations—that project from the subarachnoid space into the superior sagittal sinus for absorption of the cerebrospinal fluid into the venous system (Fig. 2.4B).
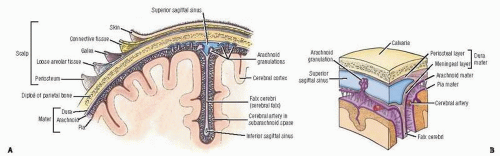 FIG. 2.4. A. Diagrammatic coronal sections through the head showing different planes, including scalp, bone, meninges, and brain. B. Diagram illustrating the relations among brain, meninges, dural sinuses, and skull. (Adapted with permission from Agur AMR, Dalley AF. Grant’s Atlas of Anatomy. 12th ed. Baltimore: Lippincott Williams & Wilkins, 2008:636.) |
The vessels at the surface of the brain are contained within the subarachnoid space; thus hemorrhages are frequent within this space (Fig. 2.4B). Dilation and congestion of the vessels at the surface of the brain are frequently observed in autopsy specimens. These findings are nonspecific and should be considered as such.
From a functional perspective, inflammatory processes and hemorrhages of the subarachnoid space have the potential to cause fibrosis of this space and hinder the normal circulation of cerebrospinal fluid and its absorption into the superior sagittal sinus. This situation may result in enlargement of the ventricular system, known as communicating hydrocephalus.
BRAIN
The brain can be divided into three major components: the cerebrum, the brainstem, and the cerebellum. Afferent and efferent connections of the brain travel in 12 pairs of cranial nerves (Fig. 2.5).
Cerebrum
The cerebrum consists of two cerebral hemispheres joined by the corpus callosum and thalamus. Each cerebral hemisphere encompasses the frontal, temporal, parietal, and occipital lobes. The external layer of the cerebral hemispheres is the cortex, a mantle of gray matter a few millimeters thick that covers large expanses of myelinated white matter. The cerebral cortex is characterized by multiple infoldings that give origin to a fairly stereotyped pattern of many plateaus (gyri) and grooves (sulci and fissures). The dorsal and lateral surfaces of the brain are known as the convexity (Figs. 2.6B and C), and the ventral surface is designated the base of the brain (Fig. 2.7). At the base of the brain, we encounter the major arteries that supply the brain and the 12 pairs of cranial nerves (Fig. 2.5, e-Fig. 2.3). In coronal sections (Figs. 2.8A-C, e-Fig. 2.4), the cerebral cortex is fairly homogeneous throughout the cerebrum, 2- to 3-mm thick, and well-demarcated from the subjacent
white matter. In the occipital lobe, the primary visual or calcarine cortex (Brodmann area 17) can easily be identified by a prominent white myelinated layer, or line of Gennari. In the mesial aspect of the temporal lobe (Fig. 2.8B), the neocortex (with six layers) is replaced by the entorhinal cortex, which merges medially into the hippocampus (Fig. 2.8C, e-Fig. 2.4). The hippocampus is an elongated structure, approximately 7 to 8 cm, wrapped in myelinated fibers that run along the temporal horn of the lateral ventricle. In coronal sections, the hippocampus is nearly round and is characterized by two interlocking lamellae of granule cells (fascia dentate) and pyramidal neurons. Immediately rostral to the hippocampus, and also abutting the temporal horn of the lateral ventricle, is the amygdala (Fig. 2.8B), a nucleus that forms part of the limbic system. At the core of the cerebral hemispheres lie several nuclei of gray matter surrounding the ventricular system (Figs. 2.8A-C). These nuclei include the basal ganglia (Figs. 2.8A and B), thalamus, and hypothalamus (e-Fig. 2.4). The basal ganglia consist of the putamen, caudate, and globus pallidum. The thalamus is a large expanse of gray matter on the banks of the third ventricle; it is bound laterally by the posterior limb of the internal capsule. The thalamus extends from its anterior nucleus, at the level of the foramina of Monro, to its most posterior nucleus or pulvinar, at the level of the splenium of the corpus callosum. Under the thalamus are two important structures: the hypothalamus and the subthalamic nucleus. The hypothalamus extends along the walls of the third ventricle, from the level of the anterior commissure rostrally to the mammillary bodies caudally. The subthalamic nucleus is a lens- or almond-shaped nucleus that occupies an oblique position under the thalamus, above the substantia nigra and lateral to the red nucleus. The ventricular system in the cerebral hemispheres encompasses the two lateral ventricles connected by the foramina of Monro to the midline third ventricle, which in turn communicates with the fourth ventricle via the aqueduct of Sylvius (Figs. 2.9A and B). Within the ventricular cavities is the choroid plexus, a richly vascularized and amorphous tissue that is attached to the ependymal lining and secretes the cerebrospinal fluid. This fluid exits the ventricular system into the subarachnoid space via two sets of foramina, Luschka and Magendie, located in the fourth ventricle.
white matter. In the occipital lobe, the primary visual or calcarine cortex (Brodmann area 17) can easily be identified by a prominent white myelinated layer, or line of Gennari. In the mesial aspect of the temporal lobe (Fig. 2.8B), the neocortex (with six layers) is replaced by the entorhinal cortex, which merges medially into the hippocampus (Fig. 2.8C, e-Fig. 2.4). The hippocampus is an elongated structure, approximately 7 to 8 cm, wrapped in myelinated fibers that run along the temporal horn of the lateral ventricle. In coronal sections, the hippocampus is nearly round and is characterized by two interlocking lamellae of granule cells (fascia dentate) and pyramidal neurons. Immediately rostral to the hippocampus, and also abutting the temporal horn of the lateral ventricle, is the amygdala (Fig. 2.8B), a nucleus that forms part of the limbic system. At the core of the cerebral hemispheres lie several nuclei of gray matter surrounding the ventricular system (Figs. 2.8A-C). These nuclei include the basal ganglia (Figs. 2.8A and B), thalamus, and hypothalamus (e-Fig. 2.4). The basal ganglia consist of the putamen, caudate, and globus pallidum. The thalamus is a large expanse of gray matter on the banks of the third ventricle; it is bound laterally by the posterior limb of the internal capsule. The thalamus extends from its anterior nucleus, at the level of the foramina of Monro, to its most posterior nucleus or pulvinar, at the level of the splenium of the corpus callosum. Under the thalamus are two important structures: the hypothalamus and the subthalamic nucleus. The hypothalamus extends along the walls of the third ventricle, from the level of the anterior commissure rostrally to the mammillary bodies caudally. The subthalamic nucleus is a lens- or almond-shaped nucleus that occupies an oblique position under the thalamus, above the substantia nigra and lateral to the red nucleus. The ventricular system in the cerebral hemispheres encompasses the two lateral ventricles connected by the foramina of Monro to the midline third ventricle, which in turn communicates with the fourth ventricle via the aqueduct of Sylvius (Figs. 2.9A and B). Within the ventricular cavities is the choroid plexus, a richly vascularized and amorphous tissue that is attached to the ependymal lining and secretes the cerebrospinal fluid. This fluid exits the ventricular system into the subarachnoid space via two sets of foramina, Luschka and Magendie, located in the fourth ventricle.
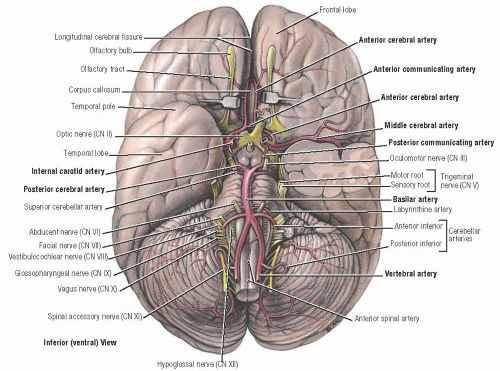 FIG. 2.5. Inferior view of the brain, demonstrating the major arteries, circle of Willis, and cranial nerves. (Reprinted with permission from Agur AMR, Dalley AF. Grant’s Atlas of Anatomy. 12th Ed. Baltimore: Lippincott Williams & Wilkins, 2008:646.) |
Brainstem
The brainstem is divided into midbrain, pons, and medulla (Fig. 2.6A). The midbrain is the most rostral division (e-Fig. 2.5). Its roof or tectum consists of the superior and inferior colliculi, immediately dorsal to the aqueducts of Sylvius, which connect the third ventricle in the cerebrum and the fourth ventricle in the pons. Other important structures in the midbrain are the periaqueductal gray matter, the nuclei of cranial nerves (CN) III and IV, substantia nigra, red nuclei, the superior cerebellar peduncles and their decussation, and the cerebral peduncles. The pons (Fig. 2.10) consists of a basal portion, or basis pontis, which contains ascending, descending, and decussating fibers, and the tegmentum, which contains the reticular activating system and the nuclei of CN V, VI, VII, and VIII. The tegmentum of the pons constitutes the floor of the fourth ventricle. The medulla contains the pyramids, inferior olivary nuclei, vestibular nuclei, and the nuclei of CN IX, X, XI, and XII.
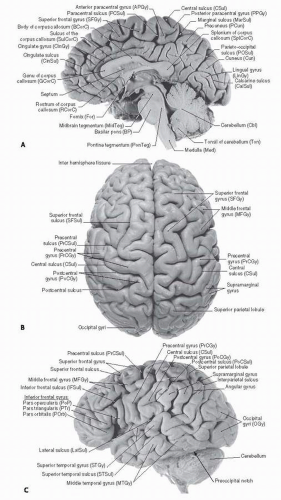 FIG. 2.6. A. Midsagittal view of the right hemi brain. B. Convexity of cerebral hemispheres, superior view. C. Lateral view of the cerebral and cerebellar hemispheres. (Reprinted with permission from Haines, DE. Neuroanatomy: An Atlas of Structures, Sections, and Systems. 6th Ed. Baltimore: Lippincott Williams&Wilkins, 2004:16, 18, 30.) |
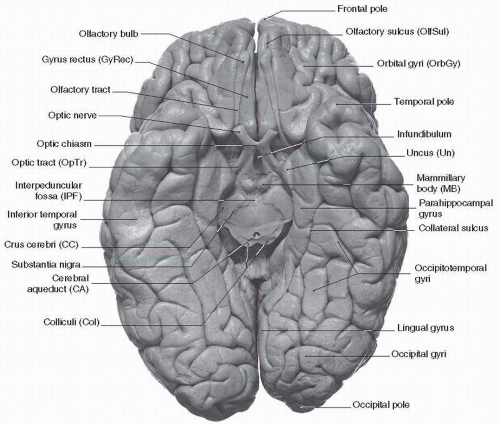 FIG. 2.7. Basal view of the cerebral hemispheres. (Reprinted with permission from Haines, DE. Neuroanatomy: An Atlas of Structures, Sections, and Systems. 6th Ed. Baltimore: Lippincott Williams & Wilkins, 2004:20.) |
Cerebellum
The cerebellum, located in the posterior fossa behind the brainstem, consists of two lateral hemispheres flanking a thin midline vermis. The surface of the cerebellum is formed by a thin layer of gray matter with thin and long infoldings that generate a pattern known as folia (Fig. 2.10). Under the folia is the white matter, abundant in the hemispheres but scant in the vermis. In the depth of the white matter lie the deep gray nuclei: dentate, globosus, emboliform, and fastigial. The dentate nucleus is the largest and the more lateral one, and is easily identified. The others are smaller, occupy more medial positions, and are better examined under themicroscope.
Cranial Nerves
The cranial nerves (Fig. 2.5) connect the brain with the body and the world. All of these nerves arise from the base of the brain, except for the cranial nerve (CN) IV pair (trochlear), which originate from the tectum of the midbrain but promptly swing around the brainstem to join the other cranial nerves at the base. All cranial nerves are peripheral nerves; thus they are myelinated by Schwann cells. An exception is the optic nerve, which is really a projection of the brain and is myelinated by oligodendrocytes.
The olfactory nerve (CN I) is composed of many tiny nerves that pierce through the cribriform plates of the ethmoid bone to reach the olfactory epithelium in the back of the nose. The olfactory nerves arise from the olfactory bulbs, which project into the cerebral cortex via the olfactory tracts. The olfactory nerves, bulbs, and tracts are frequently injured in head trauma.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


