The central nervous system (CNS) is susceptible to a number of infections caused by a broad range of pathogens. The presence of fever in the context of neurological signs or symptoms can be evidence of an underlying CNS infection. In clinical practice, the presentation may also include alteration in mental status, ranging from delirium to dementia, based on underlying etiology. Thus psychiatrists must recognize this possibility and, in the proper clinical setting, keep the diagnosis of a potential CNS infection in their differential diagnosis. In general, once the diagnosis of infection is entertained, appropriate workup includes a spinal tap for analysis of cerebrospinal fluid (CSF). The cellular and biochemical profile of the CSF varies considerably among etiologies (Table 26.1). In addition to laboratory studies, radiological studies are also frequently helpful in the investigation for a suspected infection in the CNS. The findings on computed tomography (CT) and magnetic resonance imaging (MRI) vary widely according to etiology and will be further discussed under each disease entity. With the advent of antibiotics in the middle of the last century, many CNS infections are potentially treatable. Nevertheless, the morbidity and mortality of these conditions remain high. This chapter will focus on the clinical presentation, investigation, and treatment of CNS infections.
▪ BACTERIAL MENINGITIS
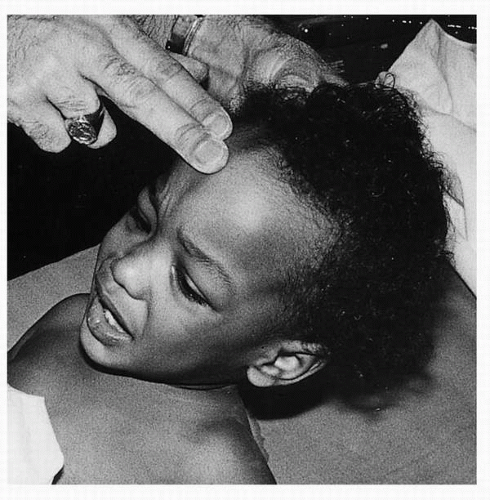
The annual incidence of bacterial meningitis is approximately 5 per 100,000 adults in the United States. Despite improved diagnostic modalities and treatment, morbidity and mortality remain relatively high. Bacteria reach the CNS by one of two routes. They may travel via hematogenous spread from another area of localized infection within the body, such as pneumonia or osteomyelitis. Alternatively, bacteria may invade the meninges by direct spread from extracranial structures, such as the middle ear or paranasal sinuses. The clinical presentation of bacterial meningitis includes the classic triad of fever, nuchal rigidity (Fig. 26.1), and altered mental status. In a large series of patients with bacterial meningitis, roughly half demonstrated the combination of these three symptoms. If headache is included in the group of presenting complaints, almost all patients with bacterial meningitis will have two of the four symptoms.
As with infections elsewhere in the body, the age of the patient, clinical setting, immune status, and evidence of systemic infection need to be taken into account when determining the organism most likely responsible for the infection (Table 26.2). Streptococcus pneumoniae and Neisseria meningitidis are the most common causative organisms in infants, children, and adults under 50 years of age. Haemophilus influenzae and Listeria monocytogenes are less common causes in this age group. In patients over 50 years old, Streptococcus pneumoniae remains the most common cause, but Listeria species and Gram-negative rods are also often seen. Newborns are susceptible to infection with Escherichia coli, group B streptococcus, and Listeria species. Nosocomial bacterial meningitis may occur in patients who have undergone a neurosurgical procedure or have sustained severe head trauma within the preceding month, have an indwelling neurosurgical device, or a CSF leak. Frequently seen organisms under these circumstances include Gram-negative rods, Staphylococcus aureus, coagulase-negative staphylococcal species, and streptococcal species.
TABLE 26.1 CEREBROSPINAL FLUID FINDINGS IN SELECTED CENTRAL NERVOUS SYSTEM INFECTIONS
DISEASE
OPENING PRESSURE
CELLS/ML
PROTEIN
GLUCOSE
OTHER STUDIES
Normal adult
6-20 cm H2O
0 PMNs <5 lymphocytes 0 RBCs
15-45
At least 50% of serum glucose
Bacterial meningitis
Normal or elevated
100-10,000 WBCs, mostly PMNs
Elevated
Less than 40% of serum glucose
Positive Gram stain or culture
Viral meningitis
Normal
10-100 WBCs, mostly lymphocytes
Normal to slightly elevated
Normal
PCR available
Viral encephalitis
Normal
10-500 WBCs, mostly lymphocytes Will see RBCs in HSV encephalitis
Normal to slightly elevated
Normal
PCR available
Toxoplasmosis
Normal or elevated
Normal to slightly elevated WBC count
Normal to slightly elevated
Normal to slightly low
PCR available
Cryptococcal meningitis
Normal or elevated
5-20 WBCs, mostly lymphocytes
Elevated
Less than 40% of serum glucose
Positive India ink stain or cryptococcal antigen titers
Tuberculous meningitis
Normal or elevated
10-1000 WBCs, PMNs early and lymphocytes later
Elevated
Less than 40% of serum glucose
Pleocytosis may be mild or absent in immunocompromised patients May see positive AFB stain or culture
Neurosyphilis
Normal
0-300 WBCs
Normal to elevated
Normal
Positive CSF VDRL Positive antitreponemal Ab
Lyme disease
Normal
10-100 WBCs, mostly lymphocytes
Normal to slightly elevated
Normal
IgM or IgG intrathecal antibody production
Neurocysticercosis
Normal
0-100 WBCs, may see eosinophils
Normal
Normal
Positive antibody
AFB, acid-fast bacilli; CSF, cerebrospinal fluid; IgG, immune globulin G; IgM, immune globulin M; PCR, polymerase chain reaction; RBCs, red blood cells; VDRL, Venereal Disease Research Laboratory; WBCs, white blood cells.
▪ FIGURE 26.1 Nuchal rigidity in a child with bacterial meningitis. (From Fleisher GR, Ludwig W, Baskin MN. Atlas of Pediatric Emergency Medicine. Philadelphia: Lippincott Williams & Wilkins; 2004.)
The workup for bacterial meningitis must be performed promptly because any delay in initiation of therapy may lead to worsened outcome. The moment the diagnosis is entertained based on clinical grounds alone, administration of antibiotics should be done before performing further diagnostic workup. The spinal tap and evaluation of CSF is the single most important diagnostic study in bacterial meningitis, and indeed in most suspected CNS infections. Before performing a spinal tap, elevated intracranial pressure (ICP) must be ruled out with appropriate imaging (usually a CT scan). A funduscopic examination is not adequate because it can take up to 2 weeks for papilledema (Fig. 26.2) to develop in cases of intracranial hypertension. Elevated ICP must be suspected if there are new-onset seizures, if the patient is immunocompromised, if there are signs on neurological examination suspicious for a space-occupying lesion, if papilledema is present, or if there is moderate to severe decrease in consciousness. If elevated ICP is present, treatment of that process as well as empiric treatment for bacterial meningitis should commence. In patients without elevated ICP, a spinal tap should be performed soon after presentation. Opening pressure, as should be measured in every spinal tap, will be high in a majority of cases of bacterial meningitis. Analysis of the CSF demonstrates a predominantly neutrophilic pleocytosis. Typically, there are 100 to 10,000 white cells per milliliter of fluid. The protein will be elevated and glucose will be decreased, less than 40% of the serum glucose when measured concomitantly. Gram stain will often demonstrate the causative organism, as will culture of the CSF. It is also useful to obtain blood cultures at the time of presentation, because they can also provide insight into the causative organism, especially if the CSF, Gram stain, or culture is negative.
TABLE 26.2 CAUSES OF BACTERIAL MENINGITIS
AGE
PATHOGENS
Newborn
Escherichia coli, group B Streptococcus, and Listeria monocytogenes
Children and adults <50 years
More common: Streptococcus pneumoniae, Neisseria meningitides Less common: Haemophilus influenzae, L monocytogenes
Adults >50 years
S pneumoniae, L monocytogenes, gram-negative rods
▪ FIGURE 26.2 Acute papilledema. (From Tasman W, Jaeger E, eds. The Wills Eye Hospital Atlas of Clinical Ophthalmology. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2001.)
As mentioned previously, early institution of broad-spectrum antibiotics can be life-saving. Studies have demonstrated a clear association between delay in starting antibiotic therapy and a high risk of adverse outcome. It is generally recommended that if imaging is performed before the spinal tap, antibiotic treatment should begin before the scan. Treatment is initially broad spectrum and can be subsequently tailored appropriately once the causative organism is identified. Usually, initial treatment includes a third-generation cephalosporin, vancomycin, and, under appropriate circumstances, ampicillin (if the patient is elderly or immunosuppressed, and therefore susceptible to infection with L monocytogenes). Recent studies have also shown that in patients with intermediate disease severity (defined as Glasgow Coma Scale score between 8 and 11) and pneumococcal meningitis, treatment with dexamethasone given shortly before or with the first dose of antibiotics and continued for 4 days reduced the incidence of adverse outcome. Therefore treatment with steroids at the time the diagnosis is entertained as often done in clinical practice.
Untreated, bacterial meningitis is almost universally fatal. Even with prompt treatment, complications of bacterial meningitis are common. In the short term, hyponatremia from the syndrome of inappropriate antidiuretic hormone (SIADH) secretion, cerebral salt-wasting syndrome, or overly aggressive fluid resuscitation may occur. As discussed earlier, increased ICP is another complication of bacterial meningitis, secondary to increased permeability of the blood-brain barrier resulting from release of proinflammatory cytokines. Acute communicating hydrocephalus has also been well-described in patients with bacterial meningitis. Seizures may occur either at presentation or after appropriate therapy and may be due to several etiologies, including increased ICP, the development of encephalitis or cerebritis, or abscess formation. Among seizure types, nonconvulsive status epilepticus has been observed in patients with bacterial meningitis, and the diagnosis must be considered in such patients when encephalopathy develops despite appropriate treatment of underlying infection and other complications. Epilepsia partialis continua (or focal motor status epilepticus) has also been described and may occur secondary to the development of subdural empyema, another potential complication of bacterial meningitis. Stroke can occur, because meningitis may lead to a septic arteritis, venous thrombophlebitis, or general thrombophilia resulting from a proinflammatory state. Nonneurological complications of meningitis occur as a result of the associated bacteremia and include septic shock, disseminated intravascular coagulation, acute respiratory distress syndrome, and septic arthritis.
The outcome of bacterial meningitis has greatly improved over the past 50 years as a result of the development of antibiotics and the improvement in prompt recognition and treatment of this condition. Nevertheless, mortality in pneumococcal meningitis ranges between 20% and 40% and 4% to 13% in meningococcal meningitis. Morbidity, in the form of either focal neurological deficits (such as hearing loss or hemiparesis) or cognitive impairment varies between 10% and 30% of survivors. The presence of coma, seizures, bacteremia, older age, and increasing number of comorbid medical illnesses at presentation are associated with a worse prognosis.
KEY POINTS
1. The clinical presentation of bacterial meningitis includes the classic triad of fever, nuchal rigidity, and altered mental status. Headache is also a very common symptom.
2.Streptococcus pneumoniae and Neisseria meningitidis are the most common causative organisms in bacterial meningitis in infants, children, and adults under the age of 50.
3. The spinal tap and evaluation of CSF is the single most important diagnostic study in bacterial meningitis, and indeed in most suspected CNS infections. Analysis of the CSF demonstrates predominantly neutrophilic pleocytosis, elevated protein, and decreased glucose level.
4. Despite improved diagnostic modalities and treatment, morbidity and mortality from bacterial meningitis remain relatively high. The workup for bacterial meningitis must be performed promptly because any delay in initiation of therapy may lead to worsened outcome.
▪ VIRAL MENINGITIS
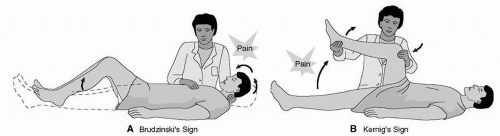
The annual incidence of viral meningitis has been reported to be roughly 20 cases per 100,000 adults in the United States. Like in bacterial meningitis, the presentation typically includes a combination of headache, fever, and meningismus. Clinically, meningismus may take the form of nuchal rigidity, pain with eye movement, or the presence of Kernig’s or Brudzinski’s signs (Fig. 26.3). Patients may also complain of photophobia, lethargy, or irritability. Clinically evident alteration in mental status, seizures, or focal neurological deficits, however, distinguishes viral meningitis from encephalitis (which will be discussed in detail later). The neurological examination is usually normal in cases of viral meningitis, but evidence of a viral infection, such as exanthema, enananthema, or evidence of other systemic involvement (e.g., pneumonia, gastroenteritis) may be present.
Viruses typically invade the CNS via hematogenous spread. Roughly 80% of cases are due to enteroviruses, including echovirus, coxsackievirus, and nonparalytic poliovirus. The peak incidence occurs in the fall months. Other causes of viral meningitis include herpes simplex virus (HSV 2, HSV 1, which more commonly causes encephalitis), varicella-zoster virus (VZV), mumps, adenovirus, human herpesvirus 6, and lymphocytic choriomeningitis virus (Table 26.3). In patients with meningitis due to HSV 2, the characteristic vesicular and ulcerative genital lesions are present approximately 85% of the time and generally precede the onset of neurological symptoms by about 1 week. The initial infection with human immunodeficiency virus (HIV) may present as aseptic meningitis or meningoencephalitis, manifested by headache, altered mental status, seizures, or cranial nerve palsies.
The characteristic findings on analysis of the CSF include a lymphocytic pleocytosis, usually with 10 to 100 cells/mL. Early in the course of the disease, neutrophils may predominate, raising concern for a bacterial process. The Gram stain will be negative in these cases, and CSF chemistry demonstrates normal to slightly elevated protein and normal glucose. There is only modest yield for identification of specific viruses based on viral cultures and specific antibody analysis. Polymerase chain reaction (PCR) for specific viruses, however, has a much better diagnostic yield and is clinically useful. Treatment of viral meningitis is largely supportive. If the underlying etiology is either HSV or VZV, treatment with acyclovir is advocated.
It should be noted that some drugs may lead to the development of aseptic meningitis, which can mimic a viral syndrome. The incidence of drug-induced aseptic meningitis is unknown, but it occurs more frequently in patients with connective tissue or autoimmune disorders. The four major classes of drugs that have been reported to cause this condition include nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics (including those used to treat various CNS infections, such as cephalosporins), muromonab-CD3 (OKT3) (an immunosuppressant agent frequently used in solid organ transplantation), and intravenous immunoglobulin (IVIG). The pathogenesis is poorly understood and is thought to be a hypersensitivity reaction. Clinically, the syndrome is indistinguishable from infectious etiologies and includes fever, meningismus, headache, and alteration in sensorium. The symptoms begin in close temporal relationship to starting the drug. The CSF profile is similar to that seen in infectious etiology, with a neutrophilic pleocytosis (100 to 1000 cells/mL) and elevated protein level. By definition, cultures are negative, and the diagnosis of drug-induced aseptic meningitis is one of exclusion. The outcome is excellent when the offending agent is withdrawn.
▪ FIGURE 26.3 Signs of meningismus: Brudzinski’s and Kernig’s signs. (From Nettina SM. The Lippincott Manual of Nursing Practice. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2001.)
TABLE 26.3 CAUSES OF VIRAL MENINGITIS AND ENCEPHALITIS
MENINGITIS
ENCEPHALITIS
–
Enteroviruses (including echovirus, coxsackievirus, and nonparalytic poliovirus)